doi: 10.56294/hl2024.413
ORIGINAL
Association between Community Engagement, Rehabilitation, and Quality of Life in Severe Mental Disorders
Asociación entre compromiso comunitario, rehabilitación y calidad de vida en trastornos mentales graves
Dhiraj Singh1 ![]() , Deepak Minhas2
, Deepak Minhas2 ![]() , Manashree Mane3
, Manashree Mane3 ![]() , Rama Sankar4
, Rama Sankar4 ![]() , Geetika M. Patel5
, Geetika M. Patel5 ![]() , Anuspandana Mahapatra6
, Anuspandana Mahapatra6 ![]() , Abhijeet Nashte7
, Abhijeet Nashte7 ![]()
1Centre of Research Impact and Outcome, Chitkara University, Rajpura, Punjab, India
2Chitkara Centre for Research and Development, Chitkara University, Himachal Pradesh, India.
3JAIN (Deemed-to-be University), Department of Forensic science, Bangalore, Karnataka, India.
4Noida International University, Greater Noida, Uttar Pradesh, India.
5Parul University, PO Limda, Tal. Waghodia, Department of Community Medicine, District Vadodara, Gujarat, India.
6IMS and SUM Hospital, Siksha ‘O’ Anusandhan (Deemed to be University), Department of Paediatrics, Bhubaneswar, Odisha, India.
7Krishna Institute of Medical Sciences, Krishna Vishwa Vidyapeeth “Deemed to be University”, Dept. of Medicine, Taluka-Karad, Dist-Satara, Maharashtra, India.
Cite as: Singh D, Deepak M, Mane M, Sankar R, Patel GM, Mahapatra A, et al. Association between Community Engagement, Rehabilitation, and Quality of Life in Severe Mental Disorders. Health Leadership and Quality of Life. 2024; 3:.413. https://doi.org/10.56294/hl2024.413
Submitted: 18-03-2024 Revised: 06-08-2024 Accepted: 09-11-2024 Published: 10-11-2024
Editor: PhD.
Prof. Neela Satheesh ![]()
ABSTRACT
Quality of life (QoL) and recovery are two widely regarded outcomes of psychiatric treatments around the world. Research highlights the potential of community involvement to enhance performance and foster progress. A survey involving 606 individuals with severe mental disorders assessed their levels of engagement, recovery, and overall satisfaction with life. The findings reveal that social involvement has a modest but statistically significant positive impact on both rehabilitation rates and general well-being. Follow-up studies further establish a correlation between recovery and life satisfaction when individuals actively participate in specific forms of engagement, with causal inferences drawn from these correlational analyses. The results suggest that emphasizing community engagement in psychological health organizations presents an opportunity to enhance rehabilitation and QoL. Research also discusses future directions, along with implications for policies and practices within the context of psychological rehabilitative initiatives.
Keywords: Health-Related Quality of Life (Hrqol), Quality of Life (Qol), Randomized Controlled Trial (RCT), Cognitive Behavioural Therapy (CBT).
RESUMEN
La calidad de vida (CdV) y la recuperación son dos resultados ampliamente considerados de los tratamientos psiquiátricos en todo el mundo. Las investigaciones destacan el potencial de la participación comunitaria para mejorar el rendimiento y fomentar el progreso. Una encuesta en la que participaron 606 personas con trastornos mentales graves evaluó sus niveles de participación, recuperación y satisfacción general con la vida. Los resultados revelan que la participación social tiene un impacto positivo modesto pero estadísticamente significativo tanto en los índices de rehabilitación como en el bienestar general. Los estudios de seguimiento establecen además una correlación entre la recuperación y la satisfacción vital cuando los individuos participan activamente en formas específicas de compromiso, con inferencias causales extraídas de estos análisis correlacionales. Los resultados sugieren que hacer hincapié en el compromiso de la comunidad en las organizaciones de salud psicológica presenta una oportunidad para mejorar la rehabilitación y la calidad de vida. La investigación también analiza las direcciones futuras, junto con las implicaciones para las políticas y prácticas en el contexto de las iniciativas de rehabilitación psicológica.
Palabras clave: Calidad de Vida Relacionada con la Salud (CVRS), Calidad de Vida (CV), Ensayo Controlado Aleatorizado (ECA), Terapia Cognitivo-Conductual (TCC).
INTRODUCTION
The term “quality of life” (QoL), the comprehension of an operation recipient’s status has grown more reliant on patient-reported measurements of the outcome, include those that evaluate health-related QoL (HRQoL) and indication associated with adverse reactions to medication. In considering such, that is important to analyze the interplay among the danger of elimination or graft loss and the toxicity of the therapy if research are to grasp the complexities of post-transplant health impacts fully.(1) More precisely, they were interested in seeing what proportion of variation in prevalence rates may be attributed to the abovementioned modifiers alongside how often it is for persons with autism to have concurrent mental disorders the condition of psycho’s spectrum disorders such as schizophrenia and bipolar spectrum disorders are additionally more common among individuals experiencing autism.(2) Utilizing a randomized controlled trial (RCT) methodology, they desired to learn whether an approach based on the diet known as the mediterranean diet affected participants’ mental health and QoL after three and six months of treatment for depression. In recognition of the low levels of omega-3 PUFAs in persons with mental illness, including in sample citation, research gave supplements made from fish oil to the patients who participated in the dietary therapy.(3) The determination and effect of variables impacting QoL in these patients are particularly relevant since QoL is becoming more prevalent in research as a patient-related consequence. Previous studies have emphasized including sociodemographic and clinical characteristics alongside the diagnosis when examining certain illness categories. Previous studies have examined crucial elements outside the diagnosis, including socio-demographic and clinical characteristics, for certain illness categories .(4) Considering this, therapies must work. These have been successful psychological therapies, particularly cognitive behavioural therapy (CBT), for bulimia nervosa and binge eating disorder (BED). However, a recent meta-analysis failed to prove that it is more effective than a placebo for treating anorexia disorder. Evidence-based therapies for severe and long-lasting instances of anorexia nervosa are for certain individuals. (5)To determine the extent to which progress has been made, this research to encourage involvement in the community has the potential to improve performance.
QoL is currently accepted by individuals’ relatives, doctors, and institutions as an intermediate and distal endpoint in therapeutic psychology.(6) The investigation has been controlled in recent decades by the diagnostic and statistical manual(DSM) and systems, with a consequent emphasis on treating presenting symptoms of mental diseases.(7) Some health-related QoL dimensions and clinically associated factors may be affected by co-occurring serious psychological disorders among male patients with drug use disorder. Therapeutic methods may need to be individualized to accommodate the variances.(8) Research that many people with mental illness, social media has become an essential division of their everyday life. Many people in this group rely on social media to discuss their struggles with mental health, get emotional and practical support from others, and learn more about available treatments, how to get in touch with mental health professionals, and how to deal with the signs they are experienced persons.(9) To develop mass and various physical health results in adults with SMI, these dietary components should be the primary objectives of preventive treatments.(10) There is an opportunity for growth in this field of research by incorporating a wider range of populations to be investigated, socially assistive robots (SARs), therapeutic applications measurements, and locations.(11) Approximately half of the people with northwest Thailand’s patients with diabetes indicated that they had a poor to average QoL. This issue may be addressed via better attention to economic problems, family support, and information regarding diabetes mellitus (DM) prevention and management and possibly the help associated with healthcare bills.(12) This provides an opportunity to examine and potentially incorporate telecommuting for rehabilitation into routine therapy by gaining experience with these digital therapies across a broad and diverse sample of patients throughout European.(13) The present investigation painted a clear and impartial depiction of social involvement among older people. The findings from the research may be used in educational institutions to help spread awareness of this idea and shape new resources. (14) The detection of these elements has revealed the difficulties of CR program implementation. Health policies should address the practical consequences of each category to increase cardiac rehabilitation (CR) implementation.(15)
METHOD
Data
Six investigations were conducted focusing on individuals with mental illnesses, resulting in data collection from 634 participants. These participants, all over the age of 16 and with a principal mental health diagnosis, were part of trials designed to assess various measures of validity and reliability in psychological tests. Participants were recruited from community mental health facilities, with a focus on inter-method reliability. Individuals with prior incarceration were also included in the sample. A randomized controlled trial (RCT) was conducted to assess the effectiveness of supporting services at a center. Research focused on the needs and benefits for individuals with severe mental illnesses, who were in the 52nd to 91st percentile of functioning. Additionally, an internet-based research initiative was launched to assess the effectiveness of parental encouragement in preventing mental health decline. Out of the initial 634 participants, 10 were excluded due to incomplete data, and 16 others were deemed unreliable due to inconsistent engagement reports. In total, the final sample consisted of 605 participants.
Measures
Participants not accompanied by staff to indicate how frequently they’ve participated in 26 activities throughout the previous thirty days. The significance of each area of engagement and the degree to which it is felt to be sufficient is also explored in the survey. The combination of all 26 components’ participation days is the total numeral of days. Each of the 11 items on the scale has a potential range of scores from 2 to 6, making them accessible to those with major mental illness. The total score was determined by adding the points earned on each item, with higher full scores indicating better QoL. There is solid evidence supporting the accuracy and reliability of the QoL questionnaire. Cronbach’s alpha for the QoL measure in this research was 0,82, respectively.
Demographics
Demographic characteristics such as the respondent’s gender, age, race/ethnicity, marital status, number of dependents, educational level, and any indicators of the respondent’s sexual orientation or gender identity person resided separately were all included in each research, whether or not they’d ever experienced homelessness. According to the framework, the total number of days spent engaging in social, productive, and recreational activities. The following is a list of items that may be found in each involvement category in society, effective contribution, and leisure participation.
Recovery Assessment Scale (RAS)
RAS, with its 19 items based on a component analysis, assessed the degree to which people felt they had recovered from their mental illness. The scale’s items gauge the respondent’s resolve, perspective, hope, ability to resist symptom dominance, and willingness to seek assistance. The total RAS score may be anywhere from 20 to 100, determined by adding the scores of the 20 subscales. A better prognosis is indicated by higher scores. Strong evidence of reliability and validity for the RAS has been identified via a thorough examination of psychometric studies. The RAS has a Cronbach’s alpha of 0,89 in this analysis.
Quality of Life (QoL) Interview
The ten-point to evaluate how people feel about their life in general, researchers at to create their QOL measure. The creation of this instrument apiece the ten questions on the scale may be responded to with a score of one or 7; the scale is designed for those with severe mental illness. Higher scores indicate better QoL, reflected in the final composite score. The validity and reliability of the QoL questionnaire have been well established. Cronbach’s alpha for the QoL measure in this research was 0,83.
The various investigations also recorded the participants’ demographic information, such as age, gender, and marital status, number of children, education, and indicators of independence/homelessness.
Analyses
Regarding the initially proposed speculation, to utilized Pearson’s correlation coefficient to examine how there was a correlation between accomplishment and satisfaction ratings and the number of days and locations of involvement the sum of time spent in various social, productive, and recreational activities. Activities, as well as their connections with RAS and QOL, were analyzed using Pearson correlations. Throughout these studies, the power source Steiger procedure for testing the significance of a difference between two dependent correlations was used. The tests were conducted using the Simple Interactive Statistical Analysis (SISA) website’s applet for analyzing overlapping correlations from a single sample.(16) The third assumption was tested by conducting a series of random-effects t-tests that compared the mean QOL and RAS scores of people who rated each participation area as essential and were involved enough with those who rated each site as important but declined to participate a sufficient amount.
RESULTS
This section presents the demographic composition, engagement metrics, and analysis of recovery and quality of life correlations, with comparisons based on gender and diagnosis using independent sample T-tests. Descriptive statistics of key variables are also summarized.
Sample description
One transgender person was included in the final sample size of 606, which included 209 males and 396 females. The mean age of the group was 44,8. Two hundred sixty-nine were in a committed relationship of some kind. Sixty-seven percent of the people surveyed were parents, either by birth or by adoption or step parenthood. One hundred fifty-eight did not have a high school diploma or equivalent, 204 did, and 244 had a college degree or higher. Three hundred ninety-eight people in the sample were self-sufficiently housed, and 326 had experienced homelessness at some time. The model had average participation duration of 71,9 days, and its participants engaged in an average of 9,3 specific activities. There was a mean of 8,2 days spent participating in social activities, 8,2 days spent working, and 16,6 days spent relaxing. Respondents ranked 17,4 different areas of engagement as vital, with 8,5 requiring at least one day of participation. There was at least one day of involvement in 51,6 % of the participation areas that were significant to respondents. There was a mean RAS score of 78,1 and a mean QOL score of 4,5. Based on the correlation, it seems that there is some similarity between the measurements, but there is also a good deal of differentiation.
Hypothesis 1: Connection between Recovery and QoL and Participation Days and Areas
Both the RAS and QOL were correlated positively with the total number of days of involvement. They weren’t distinct significantly from one another analytically. The instances of RAS and QOL were positively correlated with the respondents’ total number of involvement regions. The statistical significance of the difference between these relationships was again not established.
Hypothesis 2: The connection between recovery and QoL and participation domains
A test of significance was performed to compare the average RAS and QOL ratings of individuals that demonstrated appropriate vs. inadequate involvement in each of their most important areas of participation, and the findings are shown in the first table of this series. When comparing participants who reported high levels of engagement in all 26 of the research’s measurable involved categories to those who said poor concentration in each area, those who showed high levels of participation across the board had significantly better QOL scores. The RAS data was less stable. No discernible dissimilarity among the groups in terms of the following behaviours: grocery shopping; library use; sports-viewing; gym use; visits to a barber, attractiveness parlor, nail salon, or spa; participation in a 12-step program for substance abuse; participation in any other kind of support group; gainful employment; continued education; along with social or political involvement.
Independent sample T-test
This test outcome was given in table 1 (about the gender variability) and table 2 (based on diagnosis variability). Comparison was given in figure 1 and figure 2.
|
Table 1. Outcome Variables by Gender |
||||
|
|
Female |
Male |
||
|
|
T-Test |
T-Test |
||
|
|
Mean (M) |
Standard Deviation (SD) |
M |
SD |
|
Sense of Community |
2,34 |
0,74 |
2,59 |
0,75 |
|
Psychological Distress |
2,24 |
0,66 |
1,9 |
0,61 |
|
Mental Health Functioning |
37,86 |
10,66 |
41,36 |
10,3 |
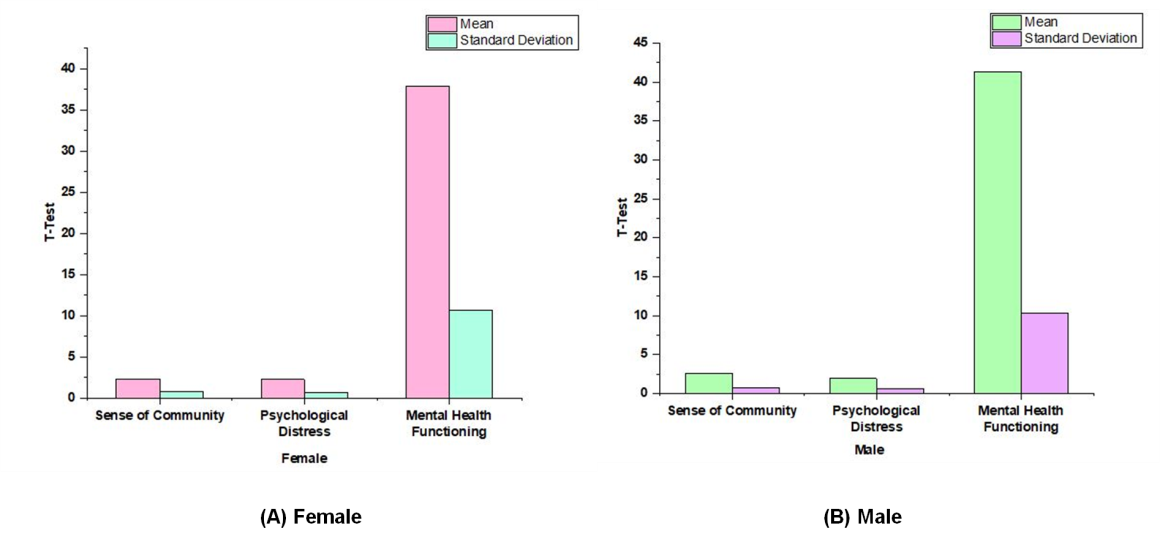
Figure 1. Result Variables by Gender (A) Female, (B) Male
|
Table 2. Result Variables by Diagnosis |
||||
|
Schizophrenia -Spectrum |
(No) |
(Yes) |
||
|
|
T-Test |
T-Test |
||
|
|
M |
SD |
M |
SD |
|
Sense of Community |
2,34 |
0,72 |
2,57 |
0,77 |
|
Psychological Distress |
2,17 |
0,68 |
2,01 |
0,63 |
|
Mental Health Functioning |
37,39 |
11,56 |
40,71 |
8,83 |
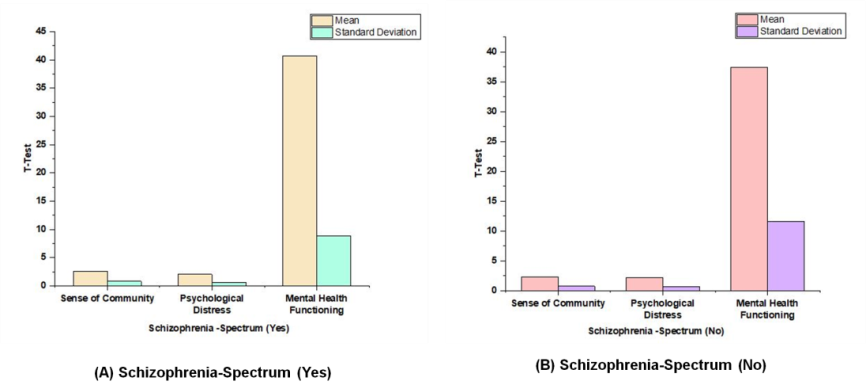
Figure 2. Comparison of Outcome Variables by Diagnosis T-Test: (A)Schizophrenia-spectrum (Yes), (B) Schizophrenia-spectrum (No)
Descriptive statistics
Table 3 and Figure 3 provides an overview of the key descriptive statistics for four variables: Community Participation, Sense of Community, Psychological Distress, and Mental Health Functioning. The range of community participation varied from 0 to 23 days, with an average of 7,57 days, indicating moderate involvement. The sense of community was scored between 2 and 5, with a mean of 2,44, suggesting a relatively lower sense of belonging. Psychological distress had a similar range, from 2 to 5, with an average score of 2,1, reflecting lower levels of distress among participants. Mental health functioning, with scores ranging from 14 to 72, had a mean of 38,8, indicating moderate mental health status overall. Figure 3 would likely provide a visual summary of these quantitative findings.
|
Table 3. Descriptive Statistics |
|||
|
|
Measure |
||
|
|
Min |
Max |
M |
|
Community Participation |
0 |
23 |
7,57 |
|
Sense of Community |
2 |
5 |
2,44 |
|
Psychological Distress |
2 |
5 |
2,1 |
|
Mental Health Functioning |
14 |
72 |
38,8 |
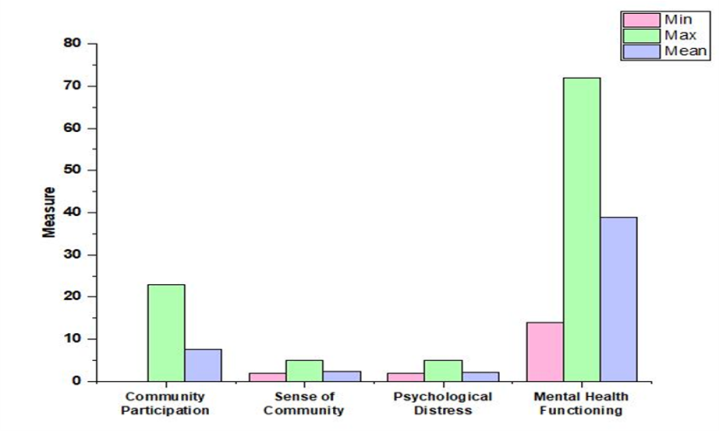
Figure 3. Quantitative Descriptions
DISCUSSION
Every one of the three hypotheses, plus the investigation’s overall premise that community engagement improves rehabilitation and QoL, is partially supported by the findings. First discovered a slight but significant correlation between total involvement days and health. It also correlated positively with progress and satisfaction in life. Second, in exploring the various participant categories; they evaluated the relative contributions of several forms of involvement to health and well-being to determine the most appropriate option. There was a weak but statistically significant positive correlation between increased levels of productive, social, and recreational activity with subsequent recovery and QoL. The strongest link between the two was the social engagement of some kind. Surprisingly, the lowest association level was found between recovery, QoL, and engagement in meaningful performance like paid or unpaid employment, education, or community service.(17) Higher ratings might be explained by the fact that the RAS and the QoL Interview place greater emphasis on social involvement than production. Eight of the ten items on the QoL scale, for instance, deal with recreational and social concerns. The RAS also includes elements that emphasize interacting with others. The productive involvement areas are highly valued by our sample, which warrants further investigation. This was determined by tallying the total number of people who responded that the area of participation was significant to them. Third, there are several important insights to be gleaned from data. The combined Ns show that at least half of respondents emphasized every kind of engagement other than watching athletics joining a civic or political organization, or going to a 12-step meeting.(18) About 80 % of people aren’t participating enough in some activities, including going to the gym, movies, or presence leisure or life ability lessons. Overall, it is evident that persons with severe mental disorders place a high value on the areas of involvement being examined. Still, they do not engage in these activities to the extent that they would want. It was expected that less rehabilitation and QoL would occur when people did not actively engage in all of these activities. QoL index was significantly correlated with involvement in 26 different activities. It indicates that being active enough in the things that matter to people may improve their QoL. Only 15 of the 26 involvement categories showed a statistically significant correlation.(19) The extent to which down the road to recovery they are substantial correlations between adequate involvement and successful recoveries were seen in the following domains. Social involvement, including going to a motion picture, a park, and entertainment the center position a theatre or cultural activity, or a social group in the community as a whole expressing belief or asking to feed help, such as visiting a mosque the service or place of worship visiting a 12-step group for the issues of mental health; or establishing a consumer-run the company. There was no correlation between adequate participation and improvement in areas like going to the store or library, watching a game, exercising, or getting a haircut. These forms of engagement may be boring. To influence the healing process, perceived adequacy in other crucial areas that lend purpose and meaning to people’s lives, such as working for income, going to school to get a diploma or degree, and engaging in civic or political activities or groups, does not seem to be associated to recovery. However, the reasons for this are unclear.(20) involvement in these areas may not have a significant effect on recovery, but this may be because people have such low expectations for involvement that even a short period, including one or two days, is seen as satisfactory and improves the quality of existence. Our findings imply that engaging with one’s community to a greater degree, particularly in areas of importance to the person, is related to a higher QoL and recovery. A possible consequence is that there needs to be a greater focus on measuring the level of neighbourhood participation of individuals with severe mental illnesses to get a clearer image of where there is the most interest in and need for involvement. Incorporating community involvement evaluations into mental health services routinely will demonstrate the need for measures to encourage more community involvement. Evidence-based practices have been established, for instance, for promoting participation in fields including housing, employment, and education; however, less focus has been placed on creating measures to increase contribution in other fields that are particularly significant to people, these “corroborates technology” that have been shown to improve competitive employment outcomes might be included in interventions to encourage more robust community engagement. Research has the obvious drawback of being purely correlational. Thus no guesses about cause and effect should be made. In other words, being well and experiencing an improved existence may make it easier for people to become involved in their communities, and conversely. More research is required to determine the nature of the connection. Additionally, despite the associations being stable and statistically significant, they are modest. The significance of community involvement in promoting health and well-being cannot be overstated. However, a second-order change or transformative change may be required to create strong, recovery-focused mental healthcare scheme around the world; the increased opportunities for community participation that would result from adopting community integration structures may indicate such an improvement.
CONCLUSION
The interaction between social contribution revival and QoL for people with severe mental diseases is complex but crucial to their health and happiness. When individuals with severe mental illnesses are actively engaged in their communities, everyone benefits. Restoring and maintaining functional capacities is the primary goal of rehabilitation, which is why it offers entire assistance and treatments. It is important to avoid having people with disabilities simply communicate with others in similarly situated categories, so it is important to develop services and supports that encourage more possibilities to enable people to participate more robustly in society. Additionally, to the degree requested by the individual, this intervention must promote self-determination and the option for engagement in areas that are essential to the personality quite than that which is for the most part convenient for organizations and services.
REFERENCES
1. Purnajo I, Beaumont JL, Polinsky M, Alemao E, Everly MJ. Trajectories of health-related quality of life among renal transplant patients associated with graft failure and symptom distress: analysis of the BENEFIT and BENEFIT-EXT trials. American Journal of Transplantation. 2020 Jun 1;20(6):1650-8. https://doi.org/10.1111/ajt.15757.
2. Lai MC, Kassee C, Besney R, Bonato S, Hull L, Mandy W, Szatmari P, Ameis SH. Prevalence of co-occurring mental health diagnoses in the autism population: a systematic review and meta-analysis. The Lancet Psychiatry. 2019 Oct 1;6(10):819-29. https://doi.org/10.1016/S2215-0366(19)30289-5
3. Parletta N, Zarnowiecki D, Cho J, Wilson A, Bogomolova S, Villani A, Itsiopoulos C, Niyonsenga T, Blunden S, Meyer B, Segal L. A Mediterranean-style dietary intervention supplemented with fish oil improves diet quality and mental health in people with depression: A randomized controlled trial (HELFIMED). Nutritional neuroscience. 2019 Jul 3;22(7):474-87. https://doi.org/10.1080/1028415X.2017.1411320
4. Berghöfer A, Martin L, Hense S, Weinmann S, Roll S. Quality of life in patients with severe mental illness: a cross-sectional survey in an integrated outpatient health care model. Quality of Life Research. 2020 Aug;29:2073-87. https://doi.org/10.1007/s11136-020-02470-0
5. van Hoeken D, Hoek HW. Review of the burden of eating disorders: mortality, disability, costs, quality of life, and family burden. Current opinion in psychiatry. 2020 Nov 1;33(6):521-7. DOI: 10.1097/YCO.0000000000000641.
6. Bobes J, Garcia-Portilla MP, Bascaran MT, Saiz PA, Bouzoño M. Quality of life in schizophrenic patients. Dialogues in clinical neuroscience. 2007 Jun 30;9(2):215-26. https://doi.org/10.31887/DCNS.2007.9.2/jbobes
7. Cuijpers P. Targets and outcomes of psychotherapies for mental disorders: an overview. World Psychiatry. 2019 Oct;18(3):276-85. https://doi.org/10.1002/wps.20661.
8. Rhee TG, Rosenheck RA. Association of current and past opioid use disorders with health-related quality of life and employment among US adults. Drug and alcohol dependence. 2019 Jun 1;199:122-8. https://doi.org/10.1016/j.jad.2022.10.025
9. Killaspy H, Harvey C, Brasier C, Brophy L, Ennals P, Fletcher J, Hamilton B. Community‐based social interventions for people with severe mental illness: a systematic review and narrative synthesis of recent evidence. World Psychiatry. 2022 Feb;21(1):96-123. https://doi.org/10.1002/wps.20940.
10. Teasdale SB, Ward PB, Samaras K, Firth J, Stubbs B, Tripodi E, Burrows TL. Dietary intake of people with severe mental illness: systematic review and meta-analysis. The British Journal of Psychiatry. 2019 May;214(5):251-9. https://doi.org/10.1192/bjp.2019.20
11. Scoglio AA, Reilly ED, Gorman JA, Drebing CE. Use of social robots in mental health and well-being research: systematic review. Journal of medical Internet research. 2019 Jul 24;21(7):e13322. https://doi.org/10.2196/13322.
12. Tamornpark R, Utsaha S, Apidechkul T, Panklang D, Yeemard F, Srichan P. Quality of life and factors associated with a good quality of life among diabetes mellitus patients in northern Thailand. Health and Quality of Life Outcomes. 2022 May 20;20(1):81. https://doi.org/10.1186/s12955-022-01986-y
13. Scherrenberg M, Wilhelm M, Hansen D, Völler H, Cornelissen V, Frederix I, Kemps H, Dendale P. The future is now: a call for action for cardiac telerehabilitation in the COVID-19 pandemic from the secondary prevention and rehabilitation section of the European Association of Preventive Cardiology. European journal of preventive cardiology. 2021 May 1;28(5):524-40. https://doi.org/10.1177/2047487320939671
14. Kaplan K, Salzer MS, Brusilovskiy E. Community participation as a predictor of recovery-oriented outcomes among emerging and mature adults with mental illnesses. Psychiatric rehabilitation journal. 2012;35(3):219. https://psycnet.apa.org/doi/10.2975/35.3.2012.219.229
15. Resurrección DM, Moreno-Peral P, Gomez-Herranz M, Rubio-Valera M, Pastor L, Caldas de Almeida JM, Motrico E. Factors associated with non-participation in and dropout from cardiac rehabilitation programmes: a systematic review of prospective cohort studies. European Journal of Cardiovascular Nursing. 2019 Jan 1;18(1):38-47. https://doi.org/10.1177/1474515118783157
16. Karlson KB, Birkelund JF. Origins of attainment: do brother correlations in occupational status and income overlap?. European Sociological Review. 2024 Jun 1;40(3):379-89. https://doi.org/10.1093/esr/jcad030
17. Rhine MA, Parrott JM, Schultz MN, Kazdoba TM, Crawley JN. Hypothesis‐driven investigations of diverse pharmacological targets in two mouse models of autism. Autism Research. 2019 Mar;12(3):401-21. https://doi.org/10.1002/aur.2066
18. Boulianne S. Twenty years of digital media effects on civic and political participation. Communication research. 2020 Oct;47(7):947-66. https://doi.org/10.1177/0093650218808186
19. Selivanova A, Fenwick E, Man R, Seiple W, Jackson ML. Outcomes after comprehensive vision rehabilitation using vision-related quality of life questionnaires: impact of vision impairment and National Eye Institute Visual Functioning Questionnaire. Optometry and Vision Science. 2019 Feb 1;96(2):87-94.10.1097/OPX.0000000000001327
20. Goldberg B, Brintnell ES, Goldberg J. The relationship between engagement in meaningful activities and quality of life in persons disabled by mental illness. Occupational Therapy in Mental Health. 2002 Mar 1;18(2):17-44. https://doi.org/10.1300/J004v18n02_03
CONFLICTS OF INTEREST
None.
FINANCING
None.
AUTHORSHIP CONTRIBUTION
Conceptualization: Dhiraj Singh, Deepak Minhas, Manashree Mane, Rama Sankar, Geetika M. Patel, Anuspandana Mahapatra, Abhijeet Nashte.
Investigation: Dhiraj Singh, Deepak Minhas, Manashree Mane, Rama Sankar, Geetika M. Patel, Anuspandana Mahapatra, Abhijeet Nashte.
Methodology: Dhiraj Singh, Deepak Minhas, Manashree Mane, Rama Sankar, Geetika M. Patel, Anuspandana Mahapatra, Abhijeet Nashte.
Writing - original draft: Dhiraj Singh, Deepak Minhas, Manashree Mane, Rama Sankar, Geetika M. Patel, Anuspandana Mahapatra, Abhijeet Nashte.
Writing - review and editing: Dhiraj Singh, Deepak Minhas, Manashree Mane, Rama Sankar, Geetika M. Patel, Anuspandana Mahapatra, Abhijeet Nashte.