doi: 10.56294/hl2024.406
ORIGINAL
Community-Based Recreation Therapy (RT) for Mental Health Recovery
Terapia recreativa comunitaria para la recuperación de la salud mental
Ashmeet Kaur1 ![]() , Abhiraj Malhotra2
, Abhiraj Malhotra2 ![]() , C.C. Khanwelkar3
, C.C. Khanwelkar3 ![]() , Roshani Majumdar4
, Roshani Majumdar4 ![]() , Geetika M. Patel5
, Geetika M. Patel5 ![]() , Mamata Devi Mohanty6
, Mamata Devi Mohanty6 ![]()
1Chitkara Centre for Research and Development, Chitkara University. Himachal Pradesh, India.
2Chitkara University Institute of Engineering and Technology, Chitkara University. Punjab, India.
3Krishna Institute of Medical Sciences, Krishna Vishwa Vidyapeeth “Deemed to be University”, Department of Pharmacology. Taluka-Karad, Dist-Satara, Maharashtra, India.
4School of Allied Health Sciences, Noida International University. Greater Noida, Uttar Pradesh, India.
5Parul University, PO Limda, Tal. Waghodia, Department of Community Medicine. District Vadodara, Gujarat, India.
6IMS and SUM Hospital, Siksha ‘O’ Anusandhan (Deemed to be University), Department of Paediatrics. Bhubaneswar, Odisha, India.
Cite as: Kaur A, Malhotra A, Khanwelkar C, Majumdar R, Patel GM, Mohanty MD. Community-Based Recreation Therapy (RT) for Mental Health Recovery. Health Leadership and Quality of Life. 2024; 3:.406. https://doi.org/10.56294/hl2024.406
Submitted: 15-03-2024 Revised: 03-08-2024 Accepted: 11-11-2024 Published: 12-11-2024
Editor: PhD.
Prof. Neela Satheesh ![]()
ABSTRACT
Community-Based Recreation Therapy (RT) is a ground-breaking and successful method that supports people in their mental health rehabilitation by using recreational activities in the community. This treatment method acknowledges the value of social interaction, leisure, and recreation in fostering overall well-being. Medication and psychosocial therapy, such as community-based RT, can help manage the signs of schizophrenia spectrum disorder (SSD), for which there is currently no recognized cure. RT offer services to persons with SSD to advance their standard of life by integrating relaxation activities and particular desires into dealing. By employing clinically validated techniques include the Mental Health Recovery (MHR) framework and suggestion from the Research Team on Patient Outcomes (RTPO), Community-Based RT has the prospect of more useful and successful in providing SSD patients with therapy in a variety of settings. The intention of this research was to examine whether recreational therapists employ clinically proven procedures by conducting a qualitative evaluation, particularly the RTPO guidelines and the principles of the MHR model, into treatment services for SSD patients. 126 RTs who presently treat or have previously treated people with SSD filled out questionnaires that gathered, processed, and reported data. Quantitative information showed that most participants use the RTPO suggestions and the MHR model’s guiding principles in their RT. Through community-based recreational activities, community-based RT provides a viable path to mental health treatment. By using examples provided by respondents to show how the concepts and proposals are applied in reality, qualitative data helped to support the quantitative findings.
Keywords: Mental Health Recovery (MHR); Schizophrenia Spectrum Disorder (SSD); Research Team on Patient Outcomes (RTPO); Community-Based Recreation Therapy (RT).
RESUMEN
La Terapia Recreativa Comunitaria (TRC) es un método innovador y exitoso que apoya a las personas en su rehabilitación de salud mental mediante el uso de actividades recreativas en la comunidad. Este método de tratamiento reconoce el valor de la interacción social, el ocio y la recreación para fomentar el bienestar general. La medicación y la terapia psicosocial, como la RT basada en la comunidad, pueden ayudar a controlar los signos del trastorno del espectro esquizofrénico (TES), para el que actualmente no existe cura reconocida. La TR ofrece servicios a las personas con TES para mejorar su nivel de vida integrando actividades de relajación y deseos particulares en el trato. Mediante el empleo de técnicas clínicamente validadas se incluye el marco de Recuperación de la Salud Mental (MHR) y la sugerencia del Equipo de Investigación sobre los Resultados de los Pacientes (RTPO), la RT basada en la comunidad tiene la perspectiva de ser más útil y exitosa a la hora de proporcionar terapia a los pacientes con SSD en una variedad de entornos. La intención de esta investigación era examinar si los terapeutas recreativos emplean procedimientos clínicamente probados mediante la realización de una evaluación cualitativa, en particular las directrices RTPO y los principios del modelo MHR, en los servicios de tratamiento para pacientes con DSS. 126 terapeutas recreativos que actualmente tratan o han tratado anteriormente a personas con DSS rellenaron cuestionarios que recogían, procesaban y comunicaban datos. La información cuantitativa mostró que la mayoría de los participantes utilizan las sugerencias de la RTPO y los principios rectores del modelo MHR en su RT. A través de actividades recreativas basadas en la comunidad, la RT basada en la comunidad proporciona un camino viable para el tratamiento de la salud mental. Mediante el uso de ejemplos proporcionados por los encuestados para mostrar cómo se aplican los conceptos y las propuestas en la realidad, los datos cualitativos ayudaron a respaldar los hallazgos cuantitativos.
Palabras clave: Recuperación de la Salud Mental (RSM); Trastorno del Espectro Esquizofrénico (TES); Equipo de Investigación sobre los Resultados de los Pacientes (RTPO); Terapia Recreativa Basada en la Comunidad (RT).
INTRODUCTION
Important epidemiological markers of disease dynamics give valuable insights into the patterns and course of illnesses within communities. Researchers, healthcare practitioners, and policymakers may get a superior perceptive of the effect that illnesses have on people and communities by using these indicators. Remission and recovery are sometimes believed to be the indications that are least well understood among them. The most well-known types of recovery are the ones that can be measured objectively, such as symptomatic recovery and functional recovery.(1) But over the last ten years, an increasing emphasis on individual rehabilitation has been promoted by people who have personally experienced it. Although there are many different ways to conceive personal healing, the following sentence captures it well. It's a manner to live a joyful, positive, and productive life while managing the boundaries imposed by illness. It, therefore, highlights the ephemeral nature of healing. MHR reports are first-person descriptions of overcoming mental health issues that make mention of occasions or deeds throughout time.(2) Figure 1 illustrates the characteristics that should be enhanced in the individual in accordance with the recovery model.
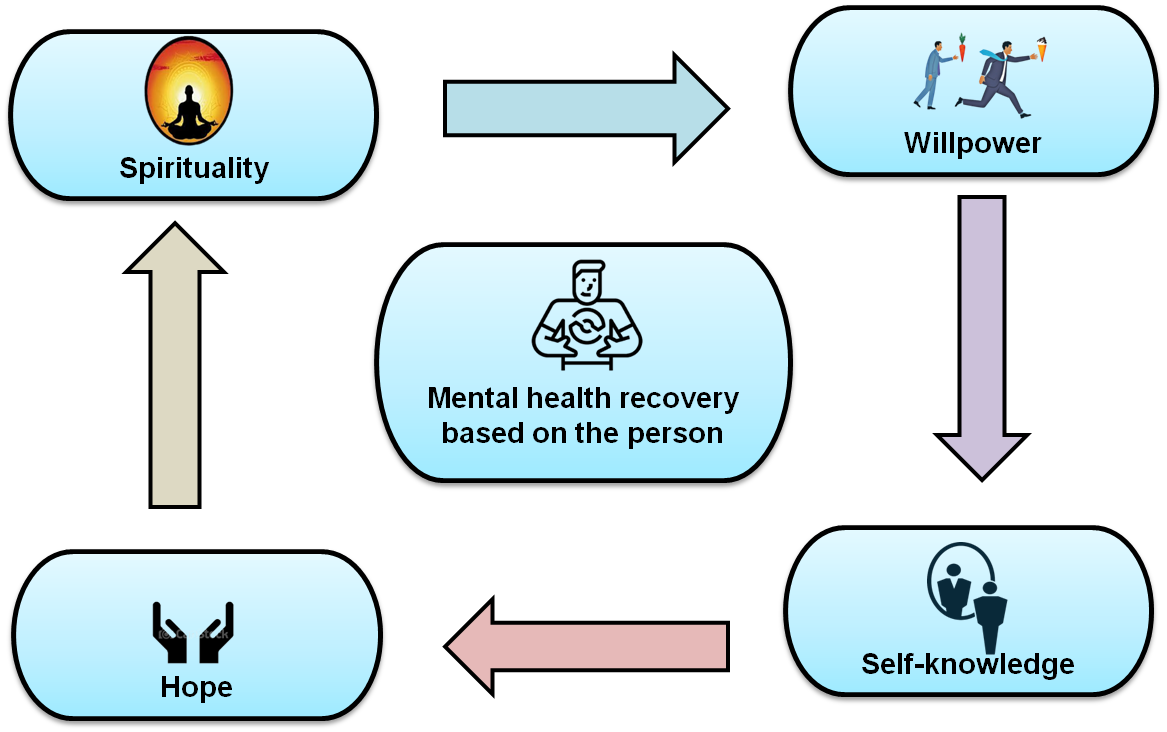
Figure 1. Individualized mental health recovery
Even though this word is also used in other areas of healthcare study and application, we will refer to them as recovery narratives for the duration of this piece. Recovery stories might be spoken aloud or recorded. In peer work, where medical instruction often supports the selective sharing of personal experiences, live rehabilitation reports are included in an ongoing connection with a client. One aspect of peer specialists' job is providing hope to others by sharing personal stories of recovery.(3) This is done by telling others about one's transformation into a hero of one's path. The failure to significantly reduce the global trouble of cerebral infirmity has led to calls for superior access to excellent cerebral health services, evaluations of mental diseases, and programs to avoid and promote mental health.
This urge for progress is fundamentally based on the difference among mental health and illness, yet this crucial distinction is often misinterpreted.(4) Traditional concepts of mental disease and mental health place them at different ends of the similar sequence, and current cerebral health treatment systems are largely built to lessen mental sickness while simultaneously enhancing cerebral health. According to certain theories, healthcare systems established in that manner run the risk of encouraging pathological avoidance, dread, and stigma in addition to providing reactive medical therapy.(5) However, that cerebral health and illness, albeit distinct, are connected but distinct conception that fall on separate spectrums. RT supports people on their path to enhanced well-being, greater self-confidence, and general mental well-being by employing recreational activities and treatments. The therapeutic advantages of leisure and recreation in fostering psychological recovery and resilience are recognized by this evidence-based approach.(6) Enhancing a person's overall quality of life is one of RT's primary goals in mental health rehabilitation. People may feel a sense of accomplishment, mastery, and personal progress by participating in fun and worthwhile activities. To effectively manage mental health issues, RT therapies put a strong emphasis on coping skill development, emotional regulation improvement, and attitude promotion.(7) In this study, we examined whether Community-Based RT treats SSD patients using evidence-based strategies, specifically the RTPO recommendations and the MHR model.
Literature review
An individual's well-being was significantly hampered by mental health. The ability to analyze text from rich resources like social media might help us better understand diseases and provide us with tools for the early identification of certain diseases. In contrast to more conventional methods,(8) used deep learning (DL) based techniques to address the problem of determining the mental state of social media users. When asked to classify a user's screen as having one of the nine ailments, the hierarchical attentive network outperforms previously defined standards for four of the nine diseases. By production scientific care accessible to infantile individuals in need, the Mental Health eClinic (MHeC) aimed to offer finest preparation of scientific therapies for those grappling with mental health difficulties.
Research(9) employed user-participatory design approaches to conduct user sessions to co-design and socially adapt to estimate the accessibility of the MHeC’s alpha prototypes, and provide guidance for the enlargement of the MHeC’s test. The COVID-19 pandemic could potentially disrupt, burden, and amplify disparities encountered. Research(10) used a mixed-methods digital assessment to review staff reports about the collision of the early COVID-19 epidemic on behavioral wellbeing services and service users. Social media, nonprofit organizations, and professional associations and networks were all utilized as recruiting tools. In addition, the study looked at the possible effects of concentration and an attachment to nature on environmental behavior. Research(11) aimed to learn more about mind-ful outdoor recreation excursions affect college students' connections to nature and conduct toward the environment. Investigated the link between meditation, a connection to nature, and ecological behavior, an explanatory mixed-method methodology was employed.
Considering the growing number of tumor survivors, such a construction might offer a way to assist timely and proper treatment. Research(12) discussed about the design of the Cancer Rehabilitation to Recreation (CaReR) construction. Physicians and other healthcare professionals could use the tailored, stepwise approach provided by the CaReR framework for developing and implementing interventions to promote regular exercise among cancer survivors. The primary purpose of virtual reality treatment was to cure phobias. Later, it was used to treat a broad variety of cerebral health issues, such as intake disorders, drug use disorders, post-traumatic stress disorder, mental disease, and autism spectrum disorders. Considering its potential to provide therapeutically useful information related to the assessment and treatment of individuals with mental illness,(13) presented a reasonable rationalization of the technique was crucial for future practice.
Signals such as temperature of the skin, blood volume pressure (BVP) and galvanic skin response (GSR) might be employed to instruct the anxiety stage organization technique. Research(14) integrated mental stress detection with virtual reality exposure therapy (VRET) and outlined various possibilities for the method. A cloud-based VRET system was developed, and one of its elements was a framework for identifying anxiety levels. Placebo-controlled clinical studies of psychedelic-assisted treatment for cerebral health issues have started to be released after a two-decade gap in that studies on psychedelics were primarily put on hold. Nine psychedelic-assisted treatments randomized, placebo-controlled clinical studies have been published,(15) examined the main endpoint standard deviation among the placebo and treatment control groups.
METHOD
In this section, the Community-Based Recreation Therapy (RT) method was discussed for MHR using RTPO Principles.
Study Design
This research engaged qualitative research using a combination of methodologies. Using a cross-sectional experiment, it was investigated whether recreational therapists include readings on the MHR model and RTPO guidelines in their treatment plans for individuals with SSD.
Techniques for Data Collection and Evaluation
The query was sent to division members in charge of mental health. Email addresses were found member database. Along with instructions on how to complete the query, participants got an explanation of the study's goals. According to the email, participating in the research is entirely up to you. Participants agree to the study's use of their information by completing the query. All of the participant-provided data was utilized only for the investigation. Also, a number of Facebook sites dedicated to Community-Based RT featured links to the study as well as a brief description of the study and its prerequisites for involvement.
Participants completed evaluations in 26 days, the program was closed. To get a high response rate during this period, the investigator used the altered Dillman approach. The link to the assessment and a cover note outlining the research were first sent to recipients in an initial email. The researcher sent a reminder email or a note of gratitude to participants who had completed the inquiry ten days after delivering the original email to those who had not responded. After then, respondents were contacted one last time. This included sending out a final appreciation to all participants, regardless of whether they filled out the inquiry or not, and informing them that the research was over.
Using SPSS and Excel, descriptive statistics were used to evaluate the analysis data. Deductive reasoning content analysis was utilized to examine the qualitative information. The following phases made up the rational content analysis procedure. First, in a Word document, each of the principles and suggestions was divided up with the matching query replies. A free-form classification matrix was then created using recurrent themes or words that supported the particular subject and were coded. Each comment was examined in a group that shared characteristics and linked to the guiding idea and suggestion. Comments that did not agree with the tenet or suggestion were discarded from the analysis. To support the concept and suggestion, a code was developed from these groupings of replies that covered the group's subject. The next step was to arrange and count the supporting words for each code to determine which code was more preventable for each particular domain.
Selection of Subjects
Participants in this research were Community-Based RT who were now treating individuals with SSD or had previously done so in an inpatient institution, a community-oriented framework, or a rehabilitation program. During one month, data collection was carried out.
Participant recruiting began after receiving approval from the IRB. Several RT groups on Facebook and relationships among the Mental Wellness Department and recreation therapists were used to find participants. Within behavioral health component are recreational therapists who practice in behavioral health settings. These environments could be inpatient psychological hospitals, which include day hospitals, intensive outpatient treatment programs, and partial hospitalization programs, co-occurring illnesses applications dependence recovery centers, forensic establishments, public educational institutions, and independent hospitalized psychiatric units within healthcare facilities. There were around 250 members in this sector who were given a chance to volunteer for the research and who got a link to the study through email.
Furthermore, the inquiry was shared on the Facebook sites of RT Foundation, RT-Acute Psych Inpatient Setting, and Therapeutic Recreation. The investigation included a snowball sample of recreational therapists who could notify other recreation therapists about the research.
Instrumentation
The research was created using the software Qualtrics since it offers question templates, enables email distribution, and reports the results of a statistical study of the responses. The unrestricted and restricted inquiries in the investigation addressed the MHR principles in Community-Based RT services for people with SSD and how RTPO's treatment recommendations were implemented. The MHR dimensions were dignity, autonomy, purity, nonlinear behavior, strengths-based, assistance from others, individualism, and person-centeredness. Furthermore, in order to treat schizophrenia and provide token economy solutions, RTPO suggested family-based activities, psychological rehabilitation instruction, professional instruction in skills, and cognitive behavioral therapy. The definition was given for each of the guidelines and suggestions as a reference. The list of definitions used in the investigation.
MHR technique principle definition: The recovery process is nonlinear, meaning it progresses with ups and downs rather than in a straight line. Empowerment is a key, ensuring that everyone involved has a voice in all treatment choices. A holistic approach is taken, addressing all aspects of the person's well-being. Recovery is self-directed, with patients actively involved in decision-making, and it is individualized and person-centered, tailoring treatment based on the patient's unique strengths, needs, and experiences.
RTPO guideline definitions: Skills training helps individuals develop or enhance abilities for everyday tasks and independent living. Family-based services involve including family and caregivers in therapy to boost social support. Vocational training provides assistance with finding and maintaining employment. Token economy interventions offer non-financial incentives for positive behavior. Community reintegration training focuses on helping individuals smoothly reintegrate into society, while cognitive behavioral therapy (CBT) teaches skills and strategies to manage and reduce distress.
The inquiry was divided into 16 areas, including six from the RTPO guidelines for treating schizophrenia and ten from the MHR model. Regarding each domain, there were two questions with Likert-style answer possibilities. The primary query was, "Do you use this principle/recommendation in your practice?" and the subsequent query was, "If so, how much?"
Respondents were asked to respond with an unrestricted statement after the Likert-type answer queries to describe how the concept or advice was used in their RT practice. The assessment included 16 Likert-style questions and nine demographic questions, which took 10 to 15 minutes to complete. Before being used in the research, the instrument underwent a pilot test with three recreational therapists to ensure the questions were relevant to the study's goals and easily understood by participants.
RESULTS
In this section, the results of Community-Based RTs with the MHR model, Quantitative and Qualitative Assessment, will be discussed. Between 26 days, Recreational Therapists who are now working with SSD patients or have in the past completed a total of 208 questionnaires through Qualtrics. As a result of the demographic questions' partial replies, around 80 results were eliminated from the total data before analysis. The finishing trial range for the research was 126 responses. The majority of participants (81,3 %) had either provided or now give RT-services to people with SSD (90,4 %). The majority of responders (29,1 %) have been dealing with SSD patients for one to three decades. The majority of respondents (67,3 %) worked in inpatient institutions, and eighty-two percent (79,4 %) held an undergraduate degree in rehabilitation therapy, or RT.
Outcomes of a Quantitative Assessment
The MHR model and the therapy suggestions made by the RTPO were discussed with the participants to gauge their familiarity with them. The replies that were given fell into three categories: highly familiar, slightly familiar, and unfamiliar. Figure 2 and 3 displays the replies to RTPO's suggestions and the MHR model.
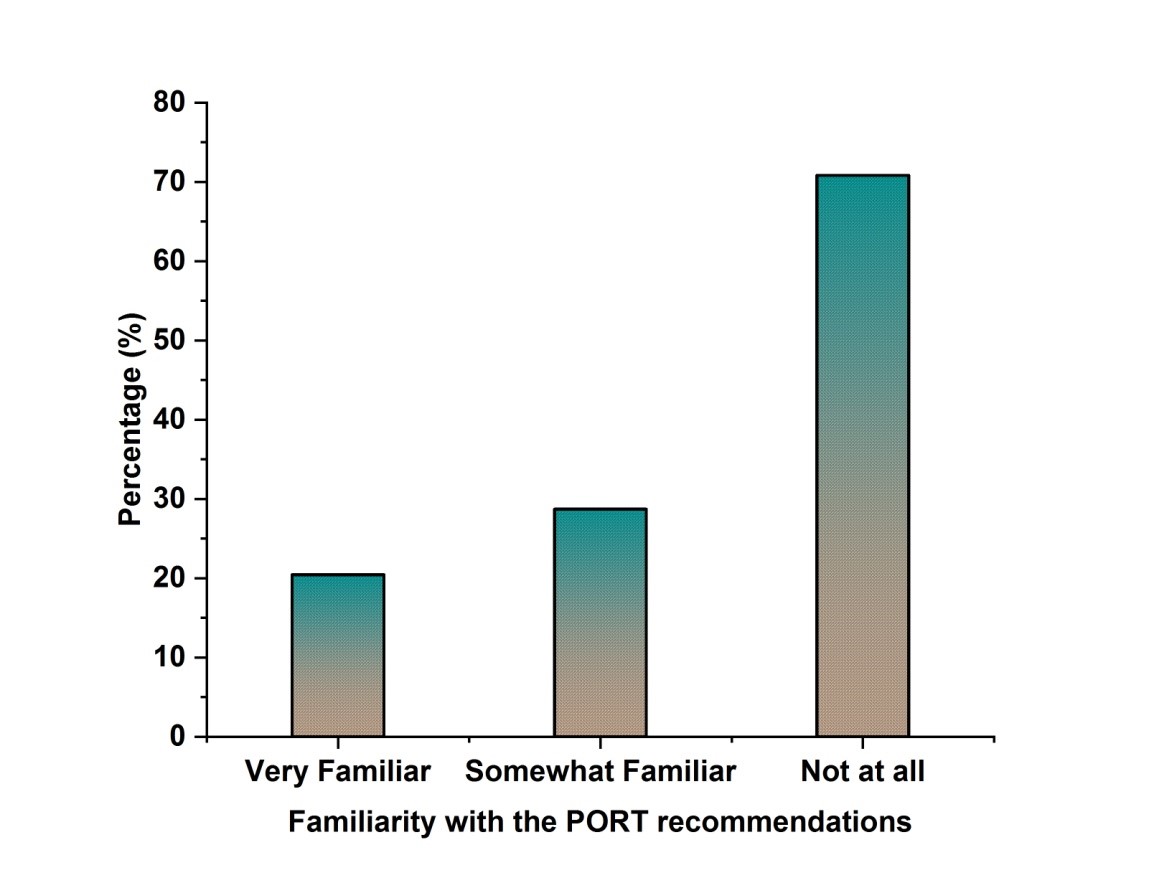
Figure 2. Involvement with the RTPO Recommendations
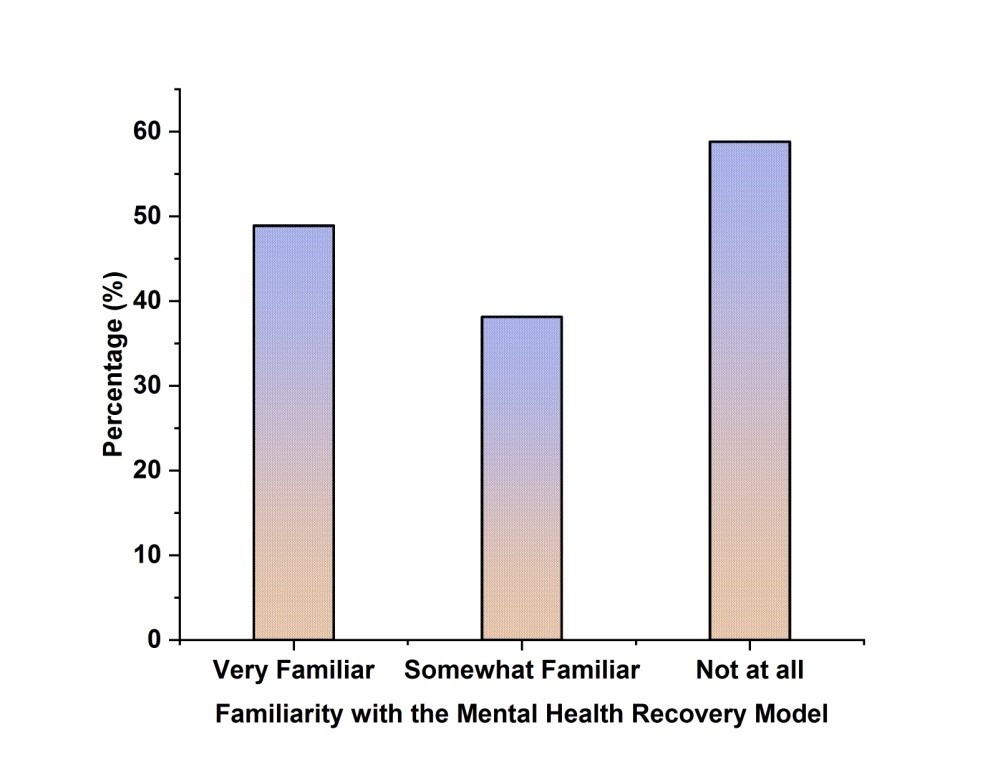
Figure 3. Involvement with the MHR model
Most respondents said they were only somewhat aware (38,12 %) of the MHR model and fully unaware of (58,8 %) of the RTPO recommendations. Analysis using cross-tabs and correlations also shows a significant correlation coefficient of r=0,408, showing that individuals who are acquainted with either the MHR model or RTPO guidelines or have a comfortable comprehension of both are included in the sample.
Principles of the MHR Model and RTPO Guidelines
To extract the answers to the query, "Is the principle/recommendation applied in practice?" separately, proportions were computed for each of the three possible responses, I don't know, No, and Yes. For ease of comparison, a mean score for every notion and suggestion was derived to determine the degree to which it is used in reality. Each answer matched with a numerical value from 1-4, table 1 and figure 4 indicate the mean calculated from the range of never, very seldom, occasionally, and a lot. According to the mean score, the following principles are listed from the most to the least applied: individualized/person-centered (3,63), holistic (3,47), nonlinear (3,37), self-direction (3,38), and empowerment (3,34). Each principle had an average rating ranging from 3,0 and 4,0, corresponding to the replies of "sometimes" and "a lot," showing that each concept is used occasionally or frequently in reality.
|
Table 1. Quantitative outcomes for the concepts in the MHR model |
|
|
Principle |
If so, how extensively is it used? |
|
Nonlinear |
3,37 |
|
Holistic |
3,47 |
|
Self-Direction |
3,38 |
|
Empowerment |
3,34 |
|
Individualized/Person Centered |
3,63 |
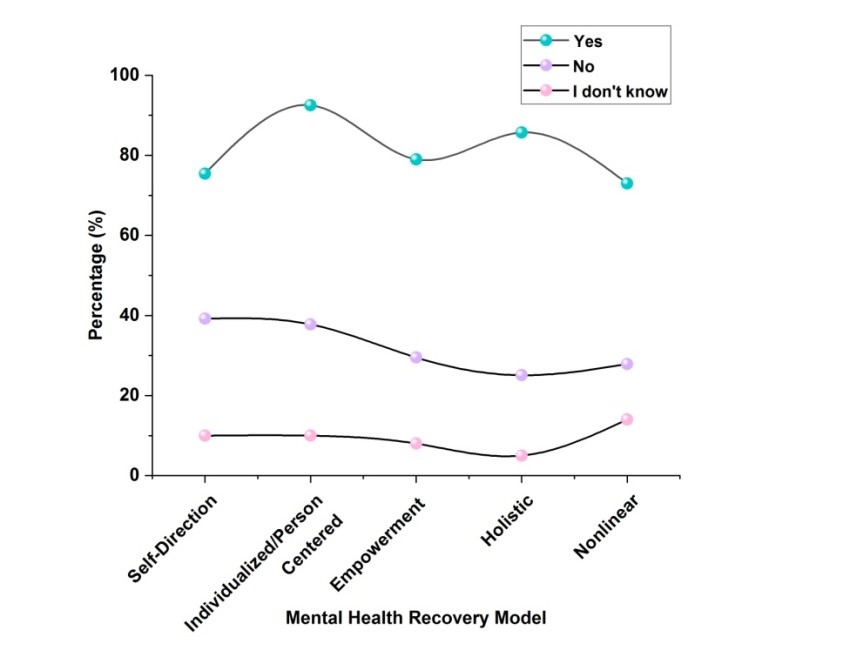
Figure 4. Quantitative findings for the principles of the MHR model
According to mean ratings, table 2 and figure 5 list the following recommendations in order of most to least popular use: skills training (3,41), Cognitive Behavioral Training (CBT) (3,60), family-based services (2,92), community reintegration training (3,02), vocational training (2,37), and token economy (2,53). When comparing the comparison between seldom and sporadically occurring in practice family-based solutions, a mean rating of 2,0 to 3,0 was given to the token economy and vocational training, respectively. Since the mean scores for these suggestions range from 3,0 to 4,0, CBT, development of skills, and social reintegration procedures are either seldom or often applied in practice.
|
Table 2. Quantitative Findings for the RTPO Recommendations |
|
|
Recommendation |
If so, how extensively is it used? |
|
Family Based Services |
2,92 |
|
Skills Training |
3,41 |
|
Token Economy |
2,54 |
|
CBT |
3,60 |
|
Community Reintegration Training |
3,02 |
|
Vocational Training |
2,37 |
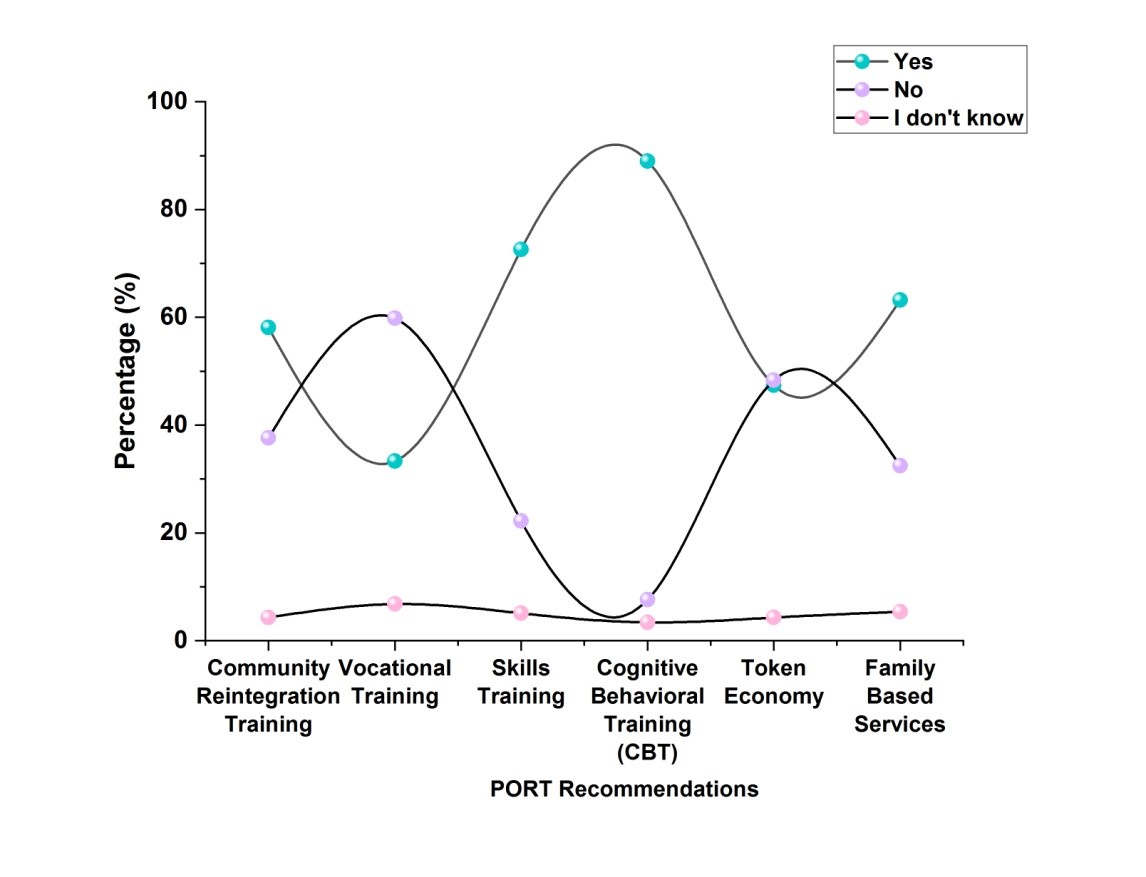
Figure 5. Quantitative Results for the RTPO Recommendations
Outcomes of a Qualitative Assessment
The deductive content evaluation was utilized to determine how the RTPO guidelines and the concepts of the MHR model are used in RT practice. According to the replies connected to the principles and suggestions, the content analysis produced a variety of codes that were then classified. The deductive content analysis is shown in table 3.
|
Table 3. Assessment of the RTPO Principles' Substance |
|
|
Recommendation |
Code (# of code occurrences) |
|
Family Based Services |
Family counseling and meetings Participating in meetings with the treatment team and learning about the therapy |
|
CBT |
Groups focus on CBT Education |
|
Skills Training |
Groups for developing different talents Resources and instruction |
|
Token Economy |
Reinforcements Prizes for group activities |
|
Community Reintegration Training |
Community assistance and knowledge about available resources Visits to therapeutic homes with family members passes, and community trips; facility tours |
|
Vocational Training |
Vocational Training Program Employment resources |
Parameters of the MHR model: Qualitative Findings
Although each of the MHR model's tenets was given separately, they were often connected. There were certain instances when codes for one principle and another overlapped. The category that most properly represented each code was given that code. Additionally, several limitations emerged in the comments, illustrating difficulties in applying the theory in reality.
Self-direction: The comment most often was that the patient's liberty in choosing interests and activities showed that their initiative is used in practice. By participating in and making decisions about different areas of therapy, as well as by applying the skill sets that are particular to each patient at the institution, self-direction is also shown in practice.
Individual and customer-focused: Assessments are often used in practice to provide tailored and person-centered treatment by gathering patient data. This idea is also implemented by tailoring the whole therapy process to each patient, using each patient's unique abilities, and giving each patient feedback.
Empowerment: The research found that giving people a chance to exercise their freedom of choice and expression is how empowerment is implemented. Through involvement and choice-making in the broader therapy process, empowerment is also pervasive throughout treatment.
Holistic: According to the study replies, this is mainly employed when creating groups to enhance a person's social, emotional, and physical well-being. Holistic therapy is also used in practice by combining many types of treatments and chances into the course of care to best enhance the superiority of life of the tolerant.
Nonlinear: According to query replies, nonlinear therapy addresses patients where they are in terms of functioning. Additionally, a nonlinear strategy is used during clinical practice by being conscious of each patient's particular cycle of symptoms and focusing on areas that may be improved during therapy. One drawback brought up in the comments is the fact that certain RT systems still treat individuals step-by-step according to the theory the program is based on.
An integrated model, the MHR model allows for the intersection and complementarity of the underlying concepts. Self-direction, accountability, people and individual focus, and empowerment are concepts that are applied in practice, and the recurrent structure of autonomy for a person was utilized to clarify the concept. Recurring codes were observed for the RTPO suggestions as well, although not as often as they were for the Recovery Model tenets. The study determining what should be included in schizophrenia therapy led to the development of the RTPO guidelines. To ensure that each patient with schizophrenia getting treatment has all the necessary skill sets and information, the guidelines are not intended to be merged but to be utilized in a specific method.
Community-Based RTs are more familiar with the MHR model and the guiding principles than with the RTPO guidelines. As a result, the principles are used in practice more often and comprehensively than the RTPO guidelines. According to examples provided by meeting individuals, the MHR model combines the RTPO proposals and uses them in conjunction with one another to allow people receiving treatment to develop the skills necessary to live freely with schizophrenia.
CONCLUSIONS
This study examines whether Community-Based RTs are providing SSD treatment services and implementing the RTPO and MHR model to those individuals. It is not obvious if programs are created around the model or suggestions, but overall participants put the ideas and recommendations into action. In Community-Based RT procedures, the Recovery Model is used more often than the RTPO guidelines. Restrictions created due to the replies may affect future research on RT procedures for SSD therapy. Although there is no known therapy for SSD, it is possible to enhance the quality of life for those diagnosed by offering care that helps them control their symptoms, lessen them, and live independently in their communities. The standard of life and promotion of MHR for SSD patients can be enhanced by incorporating the MHR framework and RTPO concepts into Community-Based RT programs.
Limitation
About 80 replies, or 38 % of the total queries, were excluded from the research because respondents started the assessment but did not respond to any of the questions, declined to participate, or did not respond to the assessment questions beyond the demographic ones. Additionally, Community-Based RTs who worked in the inpatient setting made up the bulk of the sample of participants. This may indicate that the sample does not represent RTs with these characteristics or those RTs who deal with this group often work in inpatient settings. This subject may have an impact on future studies. Additionally, RTs who work in or are affiliated with RT comprise most of the sample. Active users of social networks and organization members are among the study's respondents since it was primarily distributed via Community-Based RT Facebook pages. Even if they are qualified to participate in the study, RTs not associated with the group or the Facebook pages won't be able to access the study.
BIBLIOGRAPHIC REFERENCES
1. Morgan VA, Waterreus A, Ambrosi T, Badcock JC, Cox K, Watts GF, Shymko G, Velayudhan A, Dragovic M, Jablensky A. Mental health recovery and physical health outcomes in psychotic illness: Longitudinal data from the Western Australian survey of high impact psychosis catchments. Australian & New Zealand Journal of Psychiatry. 2021 Jul;55(7):711-28.
2. Slade M, Rennick-Egglestone S, Blackie L, Llewellyn-Beardsley J, Franklin D, Hui A, Thornicroft G, McGranahan R, Pollock K, Priebe S, Ramsay A. Post-traumatic growth in mental health recovery: qualitative study of narratives. BMJ open. 2019 Jun 1;9(6):e029342.
3. Rennick-Egglestone S, Morgan K, Llewellyn-Beardsley J, Ramsay A, McGranahan R, Gillard S, Hui A, Ng F, Schneider J, Booth S, Pinfold V. Mental health recovery narratives and their impact on recipients: systematic review and narrative synthesis. The Canadian Journal of Psychiatry. 2019 Oct;64(10):669-79.
4. Iasiello M, van Agteren J, Keyes CL, Cochrane EM. Positive mental health as a predictor of recovery from mental illness. Journal of Affective Disorders. 2019 May 15;251:227-30.
5. Charest J, Grandner MA. Sleep and athletic performance: impacts on physical performance, mental performance, injury risk and recovery, and mental health: an update. Sleep medicine clinics. 2022 Jun 1;17(2):263-82.
6. Nagata S, McCormick BP, Austin DR. Physical activity as treatment for depression in recreation therapy: Transitioning from research to practice. Therapeutic Recreation Journal. 2020 Mar 16;54(1).
7. De Vries D, Feenstra A. Making the case for recreational therapy services with individuals experiencing homelessness. World Leisure Journal. 2019 Apr 3;61(2):77-97.
8. Sekulić I, Strube M. Adapting deep learning methods for mental health prediction on social media. arXiv preprint arXiv:2003.07634. 2020 Mar 17.
9. Ospina-Pinillos L, Davenport T, Mendoza Diaz A, Navarro-Mancilla A, Scott EM, Hickie IB. Using participatory design methodologies to co-design and culturally adapt the Spanish version of the mental health eClinic: qualitative study. Journal of medical Internet research. 2019 Aug 2;21(8):e14127.
10. Johnson S, Dalton-Locke C, Vera San Juan N, Foye U, Oram S, Papamichail A, Landau S, Rowan Olive R, Jeynes T, Shah P, Sheridan Rains L. Impact on mental health care and on mental health service users of the COVID-19 pandemic: a mixed methods survey of UK mental health care staff. Social psychiatry and psychiatric epidemiology. 2021 Jan;56:25-37.
11. Deringer SA, Hanley AW, Hodges JS, Griffin LK. Improving ecological behavior in outdoor recreation through mindfulness interventions: A mixed methods inquiry. Journal of Outdoor Recreation, Education, and Leadership. 2020 May 18;12(2).
12. Dennett AM, Peiris CL, Shields N, Taylor NF. From cancer rehabilitation to recreation: a coordinated approach to increasing physical activity. Physical Therapy. 2020 Nov;100(11):2049-59.
13. Emmelkamp PM, Meyerbröker K. Virtual reality therapy in mental health. Annual review of clinical psychology. 2021 May 7;17(1):495-519.
14. Šalkevicius J, Damaševičius R, Maskeliunas R, Laukienė I. Anxiety level recognition for virtual reality therapy system using physiological signals. Electronics. 2019 Sep 16;8(9):1039.
15. Luoma JB, Chwyl C, Bathje GJ, Davis AK, Lancelotta R. A meta-analysis of placebo-controlled trials of psychedelic-assisted therapy. Journal of Psychoactive Drugs. 2020 Aug 7;52(4):289-99.
FINANCING
The authors did not receive financing for the development of this research.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORSHIP CONTRIBUTION
Data curation: Ashmeet Kaur, Abhiraj Malhotra, C.C. Khanwelkar, Roshani Majumdar, Geetika M. Patel, Mamata Devi Mohanty.
Formal analysis: Ashmeet Kaur, Abhiraj Malhotra, C.C. Khanwelkar, Roshani Majumdar, Geetika M. Patel, Mamata Devi Mohanty.
Drafting - original draft: Ashmeet Kaur, Abhiraj Malhotra, C.C. Khanwelkar, Roshani Majumdar, Geetika M. Patel, Mamata Devi Mohanty.
Writing - proofreading and editing: Ashmeet Kaur, Abhiraj Malhotra, C.C. Khanwelkar, Roshani Majumdar, Geetika M. Patel, Mamata Devi Mohanty.