doi: 10.56294/hl2024.395
ORIGINAL
Machine learning for Forecasting quality of life variations in hemodialysis patients
Aprendizaje automático para predecir variaciones en la calidad de vida de pacientes en hemodiálisis
Jamuna KV1
![]() , Uma Bhardwaj2
, Uma Bhardwaj2
![]() , Jagdish Gohil3
, Jagdish Gohil3
![]() , Jitendriya Biswal4
, Jitendriya Biswal4
![]() , Nimesh Raj5
, Nimesh Raj5
![]() , Lovish Dhingra6
, Lovish Dhingra6
![]() , V. C. Patil7
, V. C. Patil7
![]()
1JAIN (Deemed-to-be University), Department of Forensic science, Bangalore, Karnataka, India.
2Noida International University, Department of Biotechnology and Microbiology, Greater Noida, Uttar Pradesh, India.
3Parul Institute of Medical Sciences and Research, Parul University, Vadodara, Gujarat, India.
4IMS and SUM Hospital, Siksha ‘O’ Anusandhan (Deemed to be University), Department of Psychiatry, Bhubaneswar, Odisha, India.
5Centre of Research Impact and Outcome, Chitkara University, Rajpura, Punjab, India.
6Chitkara Centre for Research and Development, Chitkara University, Himachal Pradesh, India.
7Krishna Institute of Medical Sciences, Krishna Vishwa Vidyapeeth “Deemed to be University”, Dept. of Medicine, Taluka-Karad, Dist-Satara, Maharashtra, India.
Cite as: KV J, Bhardwaj U, Gohil J, Biswal J, Nimesh R, Dhingra L, et al. Machine learning for Forecasting quality of life variations in hemodialysis patients. Health Leadership and Quality of Life. 2024;3:.395. https://doi.org/10.56294/hl2024.395
Submitted: 29-03-2024 Revised: 12-08-2024 Accepted: 05-12-2024 Published: 06-12-2024
Editor: PhD.
Prof. Neela Satheesh ![]()
ABSTRACT
Objective: to anticipate changes in quality of life (QoL) evaluations for hemodialysis patients. over the course of the following month and to use ML to establish an early warning system.
Method: a hospital with a dialysis unit hosted the trial, which lasted one month and included an approaching group. Approximately 78 patients have been enrolled up to this date. Preformed including demographic information MBBS-degree holding medical professionals administered the validated WHO-BREF. It has to be done again on the same patient a month later by the same investigator. R and Orange were used for machine learning, while SPSS version 24 was used to provide basic statistics.
Results: in order to predict whether a patient’s WHO-QOL-BREF score would increase or decrease by 5 % over the course of a month, two models were developed using ML methods. A 5 % or greater loss in QOL scores occurs over the course of the next month as a result of declines in the psychosomatic, substantial, and societal domain scores.
Conclusion: the Dialysis Data Interpretation for Algorithmic-Prediction on QOL early warning system based on ML was developed to identify quickly declining QOL scores in the hemdialysis sample. The model suggested that improving the psychological and ecological domains in exacting could be able to arrest the fall in QOL ratings. If DIAL is used more widely, it should benefit patients by guaranteeing a greater QOL and reducing the long-term cost burden.
Keywords: Machine Learning (ML); Classification Tree; Quality Of Life (Qol); Hemodialysis; Prediction.
RESUMEN
Objetivo: anticipar los cambios en las evaluaciones de la calidad de vida (CdV) de los pacientes en hemodiálisis. en el transcurso del mes siguiente y utilizar la ML para establecer un sistema de alerta precoz.
Método: un hospital con una unidad de diálisis acogió el ensayo, que duró un mes e incluyó un grupo de aproximación. Hasta la fecha se han inscrito aproximadamente 78 pacientes. Preformado incluyendo información demográfica Los profesionales médicos con título de MBBS administraron el WHO-BREF validado. El mismo investigador tiene que volver a realizarlo en el mismo paciente un mes después. Se utilizaron R yOrange para el aprendizaje automático, y SPSS versión 24 para las estadísticas básicas.
Resultados: para predecir si la puntuación WHO-QOL-BREF de un paciente aumentaría o disminuiría un 5 % en el transcurso de un mes, se desarrollaron dos modelos utilizando métodos ML. Se produce una pérdida del 5 % o más en las puntuaciones de la CdV en el transcurso del mes siguiente como resultado de los descensos en las puntuaciones de los dominios psicosomático, sustancial y social.
Conclusión: se desarrolló el sistema de alerta temprana Dialysis Data Interpretation for Algorithmic-Prediction on QOL basado en ML para identificar las puntuaciones de QOL que disminuyen rápidamente en la muestra de hemodiálisis. El modelo sugirió que la mejora de los dominios psicológicos y ecológicos en la exactitud podría ser capaz de detener la caída en las puntuaciones de QOL. Si el uso de DIAL se generaliza, debería beneficiar a los pacientes al garantizar una mayor QOF y reducir la carga de costes a largo plazo.
Palabras clave: Aprendizaje Automático (ML); Árbol de Clasificación; Calidad de Vida (Qol); Hemodiálisis; Predicción.
INTRODUCTION
Possible to predict quality by applying ML on some industries such as mechanized, healthcare, and finance. Through the ML model, a piece of utensils can predict its probable date when it can be unsuccessful, by checking the sensor and supplementary sources of data. If problems can be detected in time, quality issues can be avoided by taking maintenance measures. ML can be applied to the data of the production process in order to discover some patterns which that lead to the quality problems.(1) There are a set of hyperparameters for every ML model that have to be fine-tuned for optimal performance on the validation set. Optimization can be performed through grid search, random search, or other methods, to determine the best hyperparameter combination for each model. Ensemble methods can be used to combine the predictions of multiple ML technique to enhance performance. The can involve averaging the predictions of multiple models or using more advanced techniques such as stacking or boosting.(2)
IDH is a frequent difficulty that occurs throughout hemodialysis treatment and has been linked to higher mortality rates among patients undergoing the procedure.(3) IDH is the lowering of blood pressure that occurs during hemodialysis and needs to be intervened by the health care team. The lowering of blood pressure brings with it a variety of symptoms like dizziness, giddiness, nausea, vomiting, and cramping in muscles.(4)
The shortage of kidney grafts is attributed to a number of factors, from a limited number of donor organs available to challenges in logistics at the time of organ procurement and transplantation, plus financial and regulatory barriers that have the potential of discouraging organ donation and transplantation. Moreover, a lot of things influence attitudes on organ donation culturally and religiously, which varies quite a lot within different countries and populations.(5)
These hospitalizations can be costly, not only in conditions of express medical fixed costs but also in terms of lost productivity and decreased excellence of existence for patients and their relatives.(6) Kidney damage can be indicated by abnormalities in urine tests such as the presence of protein or blood, or by imaging studies such as ultrasound or CT scans. Determining the degree to which a patient’s kidneys can filter the blood particles based on their GFR is the way through which reduced kidney function could be determined.(7) Surgeries to replace and repair structural abnormalities or injuries have been used as the first line of treatment for many health conditions for decades now. These are diseases such as heart valve dysfunction, some cancerous conditions, and joint dislocation or arthritis.(8)
Postoperative delirium is a common complication after geriatric hip fracture surgery. Delirium is a temporary state of confusion and disorientation that can occur after surgery, especially in the elderly. The incidence of delirium after geriatric hip fracture surgery has been reported to range from 10 % to 60 %.(9) The exact foundation of delirium has not been found, but the attention is laid on multiple causes, such as the effects of anesthesia and surgery, underlying medical conditions, medicines, and changed sleep patterns or circadian rhythm. Delirium can source a range of symptoms, including confusion, disorientation, hallucinations, agitation, and changes in behavior. CKD is an important healthcare weigh-down that affects millions of those worldwide. The National Kidney Foundation estimates that 10 % of the population as a whole has CKD. CKD is a degenerative illness that can proceed to ESKD, necessitating dialysis or kidney transplantation. CKD is associated with other health complications such as cardiovascular disease, anemia, and bone disease. It can also increase the risk of death, especially in individuals with comorbidities. Therefore, improving the health outcomes requires CKD prevention, early detection, and management and QOL of affected individuals.(10) ML algorithms can be used to optimize treatment plans for hemodialysis patients. For example, ML can be used to determine the optimal dialysis prescription based on a patient’s characteristics, such as grow old, influence, and comorbidities.(11)
The performance of different models can be done using a variety of metrics, including R2, but it’s significant to use numerous metrics to get an inclusive understanding of the models’ strengths and weaknesses. It would be a good performance comparison metric if mean differences between the models on the independent validation dataset were possible, since this would provide a simple measure of the average improvement one model has over the others.(12) The multiple organ systems can have long-lasting effects on a patient’s health. Therefore, there is a need for a comprehensive assessment and grading system to monitor and manage irAEs. This system will monitor patients on a regular basis concerning the progression of symptoms that occur. Detailed documentation and gradation of all adverse events reported are to be made.(13)
It involves using clinical as well as laboratory markers for recognizing the likelihood of renal flare in the patient. The can involve monitoring the patients’ serum creatinine levels, proteinuria, and other clinical markers of renal function, in addition to monitoring the illness action using measures such as the universal Lupus Erythematosus infection motion Index.(14) TIR is the percentage of time a patient’s blood sugar remains within a given range, typically between 70 to 180 mg/dL. This parameter can also be used in the measurement of the efficiency of glucose management strategies and is associated improved glucose control and lower risk of diabetes complications.(15)
The use of ML models in identifying patients with dementia represents an area of active research, and a few studies have explored the feasibility of using various types of data, including clinical and neuroimaging data, in predicting dementia in different populations of patients.(16) A machine learning technique on an updated double MQGWO combined with FKNN was implemented to test the 3069 data of 314 HD patients. The suggested MQGWO technique was validated through a few investigations such as global optimization tests, choice of feature testing using some public data sets and tests of forecasts based on an HD dataset.(17)
The performance of two MLAs trained on the task of forecasting DKD stage of severity was evaluated versus the CDC and Prevention risk score as a benchmark. Verification of the models used an independent dataset gathered from other sources together with a hold-out test set. Under the conditions of forecast correctness on the hold-out set, the techniques used obtained a area under the headset operating attribute coil (AUROC) of 0,75. (18) Considering the numerous doctor-patient and kidney transplant-related variables that influence the hemodynamic response to therapy, it is challenging to quantify in quantitative practice the risk of intradialytic adverse events with ideally balanced exclusion of appropriate solutions. Modern artificial intellect has been applied in other difficult supervisory tasks for dialysis patients and can be used for personalizing the many medicines subjecting patients’ hemodynamics to alterations during dialysis.(19) The odds of tumor control and patient survival are deteriorated by the lengthy treatment planning process, which can take up to a week, and the high degree of human skill required to generate personalized, high-quality plans. It suggested looking at the hierarchically densely connected U-net, a DL-based dosage prediction model, which is built on the two most well-liked network designs, DenseNet and U-net.(20)
Every patient undergoing maintained HD treatment at a tertiary care referral center is gathered. Medical staff members documented physiological data while HD equipment automatically gathered dialysis data. Medical professionals recorded intradialytic adverse occurrences based on patient concerns. To forecast unfavorable occurrences during HD, ML was used for features that were retrieved from time-series information sets using linear and differential analysis.(21) ML methods were additionally employed to foresee the beginning of chronic kidney failure, the progression of the disease, and the ability to survive of renal transplants in patients suffering renal diseases. For predicting chronic renal disease in the latter, RF approaches were shown to be the most effective. Decision tree models have been used in certain research to predict medication response in patients with viral illnesses, the prediction of nonalcoholic greasy liver disease, acute liver failure, and other conditions.(22)
The development of a PEPM that takes long-suffering complexity into account was another objective. An ANN was created for predicting LOS, costs, and disposition using 15 pre-operative factors from 78337 principal total hip arthroplasty patients with osteoarthritis from the general Inpatient example and the institutional database. Two criteria were utilised to determine the validity of the beneficiaries operating characteristic curve: accuracy and area under the curve. The all-patient standardised comorbid cohort was used to stratify prophetic ambiguity in order to generate the PSPM.(23) Ultimately, the study discovered that following a two-class logistic regression model comparison. Prior to beginning treatment, textural analyses were carried out on the CT scans of 72 patients in order to determine the quantitative features of intra-tumor heterogeneity.(24)
METHOD
A potential group revision (of six months) was conducted in entity of a concerned facility. Through convenience sampling with no regard to probability, patients were enrolled. There were 78 patients enrolled in all. A performance including demographic question & the validated description of the WHO-QOL-BREF are administered by a doctor with an MBBS degree. Although the raw score ranges for each domain vary, every raw score was uniformly modified to fall within the 4–20 range following WHO recommendations. A higher score indicates a higher QOL. The ultimate QOL score was created by combining the scores from all four domains. The delta QOL measured how much the overall QOL score would change during the next month. At the start of the trial, the forecaster factors were age, gender, monthly income, a monthly dosage of iron sucrose, and overall QOL score. A preliminary analysis was conducted. The foundations of a dialysis data explanation for algorithmic prediction of QOL early warning system too built based on the findings from the first interim study. The study was created exclusively for the aim of automating the publication statistics compilation of QOL scores and extra interpreter factors. Age and QOL scores are examples of continuous variables, mean and ordinary deviations were used to explain them, although percentage and frequency were used to depict unconditional variables. R and Orange were used to accomplish machine learning.
RESULTS
Results of the search process
The interim psychoanalysis comprises an entirety of 78 patients. The center age was 50,00 years (SD: 18). 53,8 % (40/75) of the total population were men. Hemodialysis treatments lasted an average of 41,40 months (SD: 25,86). At the commencement and the conclusion of the one-month episode, the mean albumin levels be 3,63 g/dl (SD=1,43) and 2,54 g/dl (SD=2,50), correspondingly which correspondingly as shown in table 1.
|
Table 1. Specifications of the variables examined |
||||||
|
|
Overall |
|
Men |
|
Women |
|
|
Variables |
Mean |
SD |
Mean |
SD |
Mean |
SD |
|
Age |
52 |
22 |
56 |
22 |
49 |
25 |
|
DOM1-Physical Change2 |
0,42 |
2,71 |
0,35 |
3,11 |
0,50 |
2,18 |
|
(g/dl) Hemoglobin -end |
10,08 |
1,59 |
10,09 |
1,89 |
10,06 |
1,15 |
|
(g/dl) Hemoglobin -start |
10,44 |
1,73 |
10,58 |
1,87 |
10,27 |
1,83 |
|
Hemodialysis Duration |
41,42 |
28,94 |
47,52 |
31,33 |
34,32 |
24,53 |
|
(g/dl) Albumin -end |
3,65 |
0,56 |
3,72 |
0,59 |
3,58 |
0,52 |
|
(g/dl) Albumin -start |
3,63 |
0,56 |
3,68 |
0,59 |
3,58 |
0,51 |
|
DOM2-Psychological Change2 |
1,03 |
2,78 |
1,64 |
2,94 |
0,32 |
2,42 |
|
DOM3-Social Change2 |
0,24 |
3,55 |
-0,18 |
3,91 |
-0,32 |
3,12 |
|
QOL Total score-start |
57,63 |
10,36 |
58,99 |
11,09 |
56,04 |
9,35 |
|
QOL Change2 |
1,73 |
7,68 |
2,49 |
8,62 |
0,84 |
6,41 |
|
QOL Total score-end |
59,35 |
10,28 |
61,44 |
9,09 |
56,86 |
11,13 |
|
DOM4-Environmental Change2 |
0,55 |
2,75 |
0,70 |
3,13 |
0,37 |
2,23 |
To determine if there is a comparable difference between the sexes, many student t-tests were run, as shown in table 2 and figure 1. It demonstrated a substantial difference between men and females in terms of the mean score of psychosomatic categories and the total QOL score. The relative scores of men were higher.
|
Table 2. Hemodialysis patients’ QOL domain scores vary between men and women |
||
|
Variables |
Mean Difference |
Significance |
|
Physical- DOM1 |
-1,1 |
0,21 |
|
Psychological- DOM2 |
-1,8 |
0,046 |
|
Social- DOM3 |
-1,3 |
0,087 |
|
Environmental- DOM4 |
-1,3 |
0,085 |
|
QOL Total Score |
-4,8 |
0,049 |
|
QOL Change Score |
-1,62 |
0,37 |
After that, a linear degeneration reproduction was fitted (p<0,001,r2=0,418). To create a model, factors such as age, gender, monthly income, the digit of months spent receiving hemodialysis, and change in the principles of variables such as serum albumin, potassium, calcium, phosphate, and hemoglobin be taken into consideration. The termination variable chosen was the overall shift in the QOL score as a whole. As demonstrated in Table 3 and Figure 2, Higher QOL was shown to have a strong positive correlation between serum albumin (p<0,001) and monthly income (p<0,001).
The arrangement hierarchy was determined to be the most exact model, with a district underneath curvature (AUC) of 83,3 % (accuracy: 81,9 %) for the forecast of a 5 % rise in QOL over the next month and an AUC of 76,2 % (accuracy: 81,8 %) for the forecast of a 5 % reduction over the same period.
In order of significance, a decline in domain two (psychosomatic), one (substantial), and three (societal) as well as higher legion research were correlated with a 5 % reduction as shown in figure 3.
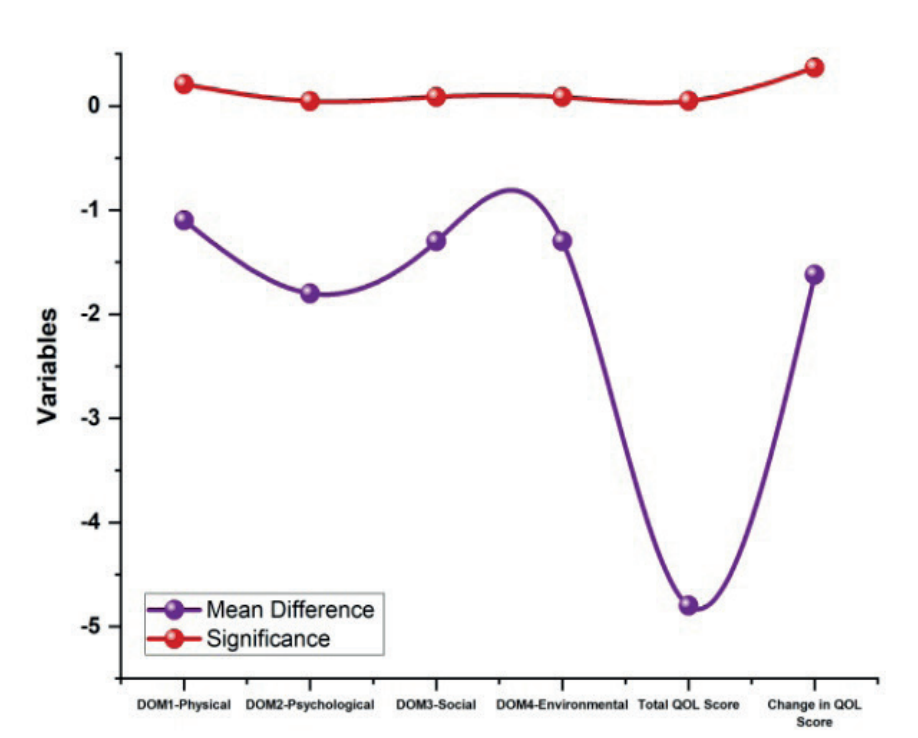
Figure 1. QOL domain ratings vary in hemodialysis patients
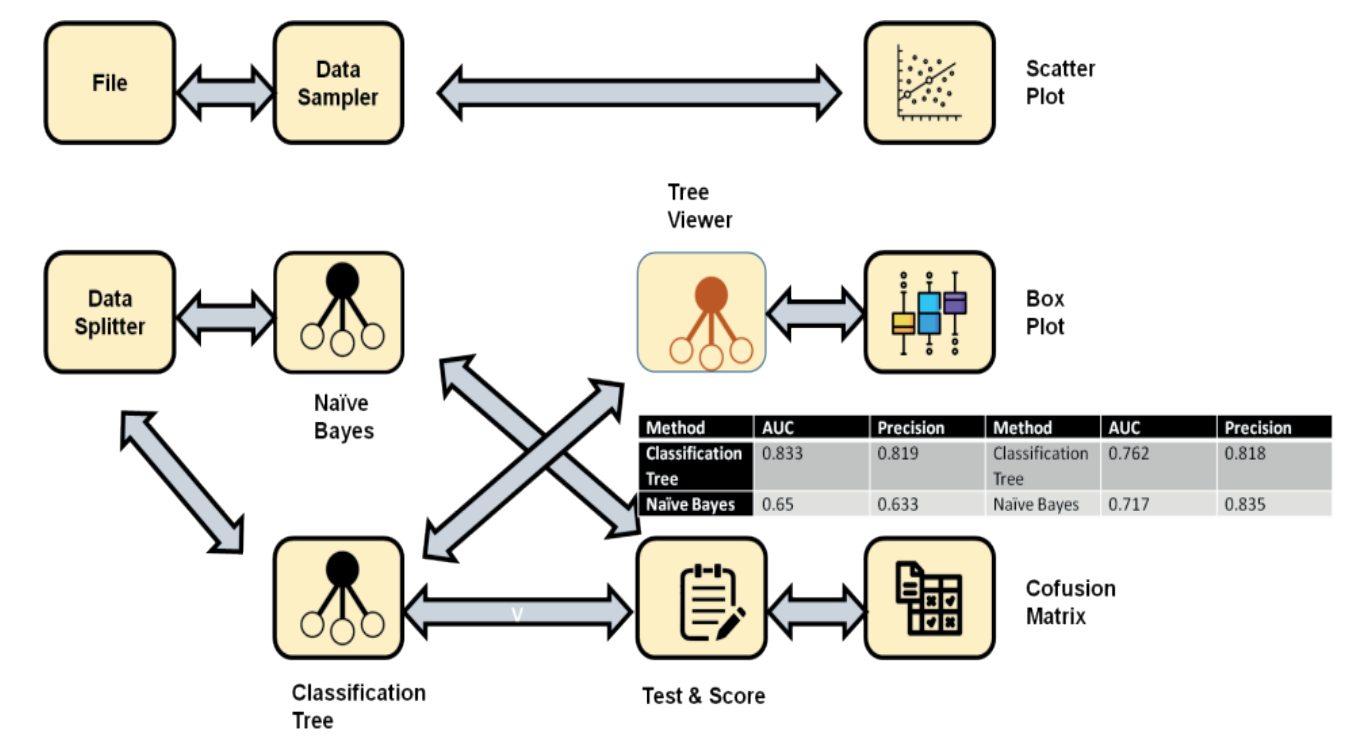
Figure 2. ML method applied to both prediction models using confusion matrices
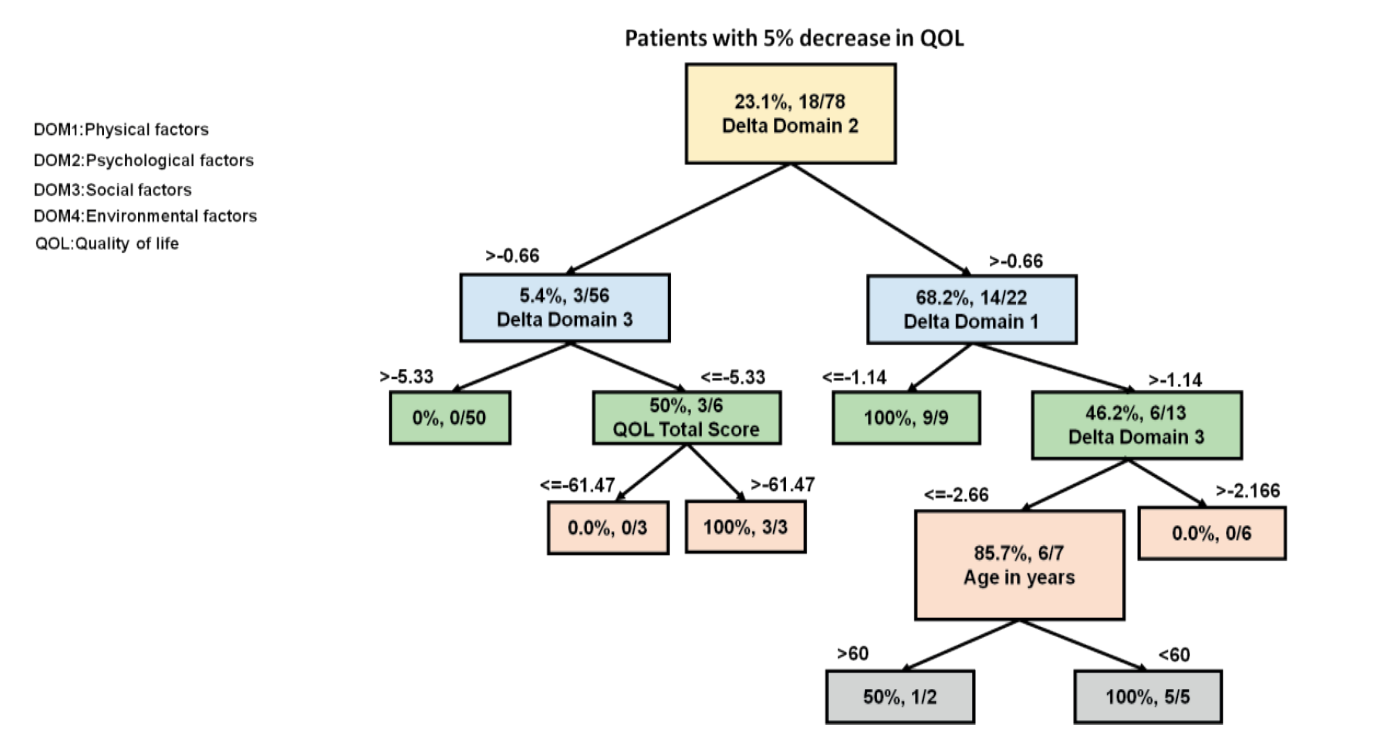
Figure 3. Classification tree variables affecting QOL scores by 5 % or more
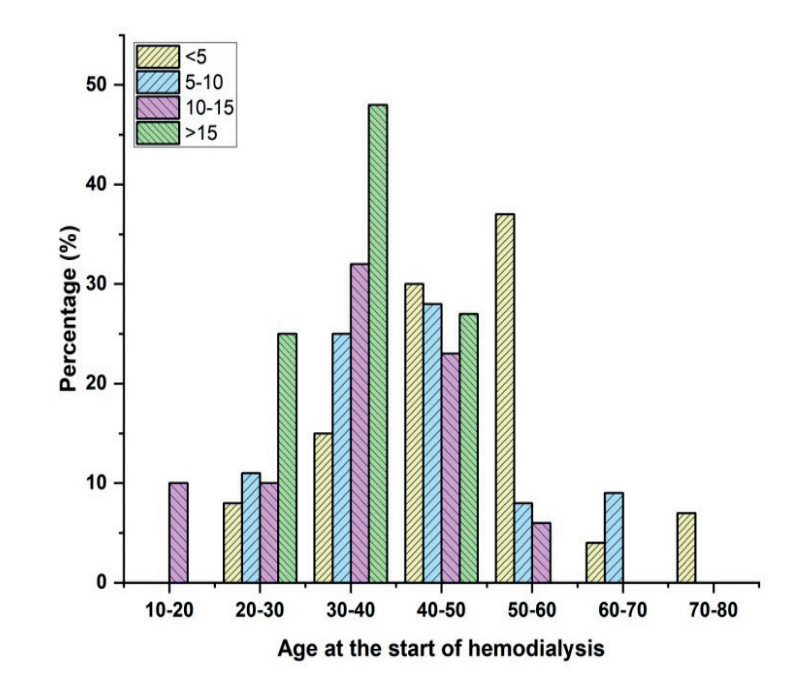
Figure 4. By age group, the proportions of patients having different hemodialysis durations
Patients undergoing hemodialysis for fewer than five years, ages 25 to 82, are shown in Figure 4. Patients who had been receiving hemodialysis for five to ten years ranged in age from 21 to 74 at the beginning of treatment. The patients receiving hemodialysis for 10–15 years varied in age from 14 to 67 when treatment started. The age range of patients receiving hemodialysis for more than 15 years was 26 to 47. The linear regression analysis’s coefficients graph is shown in figure 5.
|
Table 3. Coefficients of linear regression |
||
|
Variable |
Significance |
B1 |
|
Income per family |
0,002 |
4,54 |
|
Age |
0,155 |
-0,1 |
|
Calcium |
0,272 |
-1,57 |
|
Hemoglobin |
0,402 |
0,58 |
|
Phosphate |
0,55 |
0,33 |
|
Constant |
0,031 |
27,37 |
|
Income per family |
0,002 |
4,54 |
|
Gender |
0,494 |
1,47 |
|
Potassium |
0,684 |
-0,47 |
|
Months on HD |
0,312 |
-0,06 |
|
Albumin |
0,002 |
8,16 |
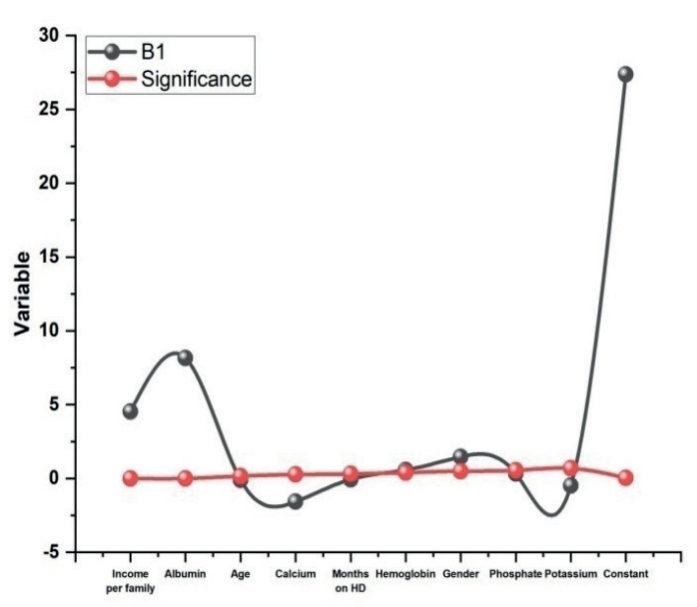
Figure 5. Coefficients graph for linear regression analysis
DISCUSSION
Patients undergoes hemodialysis make up a unique demographic. Many people experience some amount of despair after learning they have an ESRD. Their entire QOL is affected by physical, social, and psychological factors, which are reflected in their lives. To classify patients who are at an elevated threat of losing their QOL scores and focus recovery efforts on certain areas. Using the WHOQOL-BREF Urdu questionnaire, it gathered information at an Islamabad facility on the most important variables that could have an impact on QOL scores in hemodialysis populations. It was successful in creating a forecast representation by using contemporary ML techniques. There is no precedent for developing a DIAL-like early warning system, which might eventually be utilized as a monthly surveillance system to identify and priorities patients who are most at chance of witnessing a drop in QOL ratings within the following month.
There are additional sectors where the kind of technology is used. Advanced iron substitute dosages were shown to be related to higher QOL ratings in the research. Since the highest intravenous dosage administered was 800 mg per month, it was unable to determine whether or not doses higher than 800 mg are linked to a decline in QOL ratings. Other studies have identified the best iron replacement dosages for clinical hemoglobin improvement and, by extension, for relieving clinical symptoms. The dimensions changed whose QOL ratings declined. These changes were the major causes of this outcome. Patients who were older but less than sixty years old were more likely to see a decline in QOL ratings during the next month.
This could be related to the fact that compared to elderly greater than sixty and younger thirty populations, middle-aged patients experience more limitations and restrictions as a result of dialysis earlier in life. The research has several drawbacks as well. Additionally, the majority of QOL-related questions were based on one’s subjective assessment. Despite the convenience sampling and reduced sample size, the considerable AUC values and high accuracy point to a very reliable and consistent prediction and monitoring system. As a consequence, it team decides to publish the interim findings. It institution is using the DIAL screening/surveillance system. If DIAL lessens the long-term cost burden on dialysis patients that are what we want to learn. Doctors’ decision-making will be aided by the use of ML methods in the healthcare industry. It is anticipated that would give clinicians greater confidence to treat their patients effectively.
CONCLUSION
In this work, it used ML techniques to develop DIAL, an early warning system for the hemodialysis population to detect a fall in QOL scores early on. With an AUC of 83,3 %, the research was talented to recognize a segment of the hemodialysis inhabitants that was most at risk for this decline. To stop this decrease, the model also recommended focusing in particular on the psychosomatic & ecological domains. DIAL is anticipated to benefit patients by providing a higher QOL and a long-term decrease in financial load if it is deployed on a bigger scale.
REFERENCES
1. Huang JC, Tsai YC, Wu PY, Lien YH, Chien CY, Kuo CF, Hung JF, Chen SC, Kuo CH. Predictive modeling of blood pressure during hemodialysis: A comparison of linear model, random forest, support vector regression, XGBoost, LASSO regression and ensemble method. Computer methods and programs in biomedicine. 2020 Oct 1;195:105536. https://doi.org/10.1016/j.cmpb.2020.105536
2. Burlacu A, Iftene A, Jugrin D, Popa IV, Lupu PM, Vlad C, Covic A. Using artificial intelligence resources in dialysis and kidney transplant patients: a literature review. BioMed research international. 2020;2020(1):9867872. https://doi.org/10.1155/2020/9867872
3. Qiu Y, Huang Y, Wang Y, Ren L, Jiang H, Zhang L, Dong C. The role of socioeconomic status, family resilience, and social support in predicting psychological resilience among Chinese maintenance hemodialysis patients. Frontiers in Psychiatry. 2021 Sep 30;12:723344. https://doi.org/10.3389/fpsyt.2021.723344
4. Ferguson TW, Whitlock RH, Bamforth RJ, Beaudry A, Darcel J, Di Nella M, Rigatto C, Tangri N, Komenda P. Cost-utility of dialysis in Canada: hemodialysis, peritoneal dialysis, and nondialysis treatment of kidney failure. Kidney medicine. 2021 Jan 1;3(1):20-30. https://doi.org/10.1016/j.xkme.2020.07.011
5. Sukul N, Karaboyas A, Csomor PA, Schaufler T, Wen W, Menzaghi F, Rayner HC, Hasegawa T, Al Salmi I, Al-Ghamdi SM, Guebre-Egziabher F. Self-reported pruritus and clinical, dialysis-related, and patient-reported outcomes in hemodialysis patients. Kidney medicine. 2021 Jan 1;3(1):42-53. https://doi.org/10.1016/j.xkme.2020.08.011
6. Tommel J, Evers AW, van Hamersvelt HW, Jordens R, van Dijk S, Hilbrands LB, van Middendorp H, E-HELD Study Group. Predicting health-related quality of life in dialysis patients: factors related to negative outcome expectancies and social support. Patient Education and Counseling. 2021 Jun 1;104(6):1474-80. https://doi.org/10.1016/j.pec.2020.11.019
7. Savić M, Kurbalija V, Ilić M, Ivanović M, Jakovetić D, Valachis A, Autexier S, Rust J, Kosmidis T. The application of machine learning techniques in prediction of quality of life features for cancer patients. Computer Science and Information Systems. 2023;20(1):381-404. https://doi.org/10.2298/CSIS220227061S
8. Senanayake S, White N, Graves N, Healy H, Baboolal K, Kularatna S. Machine learning in predicting graft failure following kidney transplantation: A systematic review of published predictive models. International journal of medical informatics. 2019 Oct 1;130:103957. https://doi.org/10.1016/j.ijmedinf.2019.103957
9. Senanayake S, White N, Graves N, Healy H, Baboolal K, Kularatna S. Machine learning in predicting graft failure following kidney transplantation: A systematic review of published predictive models. International journal of medical informatics. 2019 Oct 1;130:103957. https://doi.org/10.1016/j.ijmedinf.2019.103957
10. Chaudhuri S, Han H, Usvyat L, Jiao Y, Sweet D, Vinson A, Steinberg SJ, Maddux D, Belmonte K, Brzozowski J, Bucci B. Machine learning directed interventions associate with decreased hospitalization rates in hemodialysis patients. International Journal of Medical Informatics. 2021 Sep 1;153:104541. https://doi.org/10.1016/j.ijmedinf.2021.104541
11. Baumbach L, List M, Grønne DT, Skou ST, Roos EM. Individualized predictions of changes in knee pain, quality of life and walking speed following patient education and exercise therapy in patients with knee osteoarthritis–A prognostic model study. Osteoarthritis and Cartilage. 2020 Sep 1;28(9):1191-201. https://doi.org/10.1016/j.joca.2020.05.014
12. Iivanainen S, Ekstrom J, Virtanen H, Kataja VV, Koivunen JP. Electronic patient-reported outcomes and machine learning in predicting immune-related adverse events of immune checkpoint inhibitor therapies. BMC Medical Informatics and Decision Making. 2021 Dec;21:1-8. https://doi.org/10.1186/s12911-021-01564-0
13. Chen Y, Huang S, Chen T, Liang D, Yang J, Zeng C, Li X, Xie G, Liu Z. Machine learning for prediction and risk stratification of lupus nephritis renal flare. American Journal of Nephrology. 2021 Jul 12;52(2):152-60. https://doi.org/10.1159/000513566
14. Deng Y, Lu L, Aponte L, Angelidi AM, Novak V, Karniadakis GE, Mantzoros CS. Deep transfer learning and data augmentation improve glucose levels prediction in type 2 diabetes patients. NPJ Digital Medicine. 2021 Jul 14;4(1):109. https://doi.org/10.1038/s41746-021-00480-x
15. Lee R, Choi H, Park KY, Kim JM, Seok JW. Prediction of post-stroke cognitive impairment using brain FDG PET: deep learning-based approach. European Journal of Nuclear Medicine and Molecular Imaging. 2022 Mar 1:1-9. https://doi.org/10.1007/s00259-021-05556-0
16. Yang X, Zhao D, Yu F, Heidari AA, Bano Y, Ibrohimov A, Liu Y, Cai Z, Chen H, Chen X. An optimized machine learning framework for predicting intradialytic hypotension using indexes of chronic kidney disease-mineral and bone disorders. Computers in Biology and Medicine. 2022 Jun 1;145:105510. https://doi.org/10.1016/j.compbiomed.2022.105510
17. Hu J, Liu Y, Heidari AA, Bano Y, Ibrohimov A, Liang G, Chen H, Chen X, Zaguia A, Turabieh H. An effective model for predicting serum albumin level in hemodialysis patients. Computers in Biology and Medicine. 2022 Jan 1;140:105054. https://doi.org/10.1016/j.compbiomed.2021.105054
18. Barbieri C, Cattinelli I, Neri L, Mari F, Ramos R, Brancaccio D, Canaud B, Stuard S. Development of an artificial intelligence model to guide the management of blood pressure, fluid volume, and dialysis dose in end-stage kidney disease patients: proof of concept and first clinical assessment. Kidney diseases. 2019 Feb 1;5(1):28-33. https://doi.org/10.1159/000493479
19. Hiramatsu R, Ubara Y, Sawa N, Sakai A. Hypocalcemia and bone mineral changes in hemodialysis patients with low bone mass treated with denosumab: a 2-year observational study. Nephrology Dialysis Transplantation. 2021 Oct 1;36(10):1900-7. https://doi.org/10.1093/ndt/gfaa359
20. Liu YS, Yang CY, Chiu PF, Lin HC, Lo CC, Lai AS, Chang CC, Lee OK. Machine learning analysis of time-dependent features for predicting adverse events during hemodialysis therapy: Model development and validation study. Journal of Medical Internet Research. 2021 Sep 7;23(9):e27098. https://doi.org/10.2196/27098
21. Saberi-Karimian M, Khorasanchi Z, Ghazizadeh H, Tayefi M, Saffar S, Ferns GA, Ghayour-Mobarhan M. Potential value and impact of data mining and machine learning in clinical diagnostics. Critical reviews in clinical laboratory sciences. 2021 May 19;58(4):275-96. https://doi.org/10.1080/10408363.2020.1857681
22. Greenwood SA, Koufaki P, Macdonald JH, Bhandari S, Burton JO, Dasgupta I, Farrington K, Ford I, Kalra PA, Kean S, Kumwenda M. Randomized trial—prescription of intradialytic exercise to improve quality of life in patients receiving hemodialysis. Kidney International Reports. 2021 Aug 1;6(8):2159-70. https://doi.org/10.1016/j.ekir.2021.05.034
23. Tran NK, Sen S, Palmieri TL, Lima K, Falwell S, Wajda J, Rashidi HH. Artificial intelligence and machine learning for predicting acute kidney injury in severely burned patients: a proof of concept. Burns. 2019 Sep 1;45(6):1350-8. https://doi.org/10.1016/j.burns.2019.03.021
24. Moghadas-Dastjerdi H, Sha-E-Tallat HR, Sannachi L, Sadeghi-Naini A, Czarnota GJ. A priori prediction of tumour response to neoadjuvant chemotherapy in breast cancer patients using quantitative CT and machine learning. Scientific Reports. 2020 Jul 2;10(1):10936. https://doi.org/10.1038/s41598-020-67823-8
FINANCING
None.
CONFLICT OF INTEREST
None.
AUTHORSHIP CONTRIBUTION
Conceptualization: Jamuna KV, Uma Bhardwaj, Jagdish Gohil, Jitendriya Biswal, Nimesh Raj, Lovish Dhingra, V. C. Patil.
Data curation: Jamuna KV, Uma Bhardwaj, Jagdish Gohil, Jitendriya Biswal, Nimesh Raj, Lovish Dhingra, V. C. Patil.
Formal analysis: Jamuna KV, Uma Bhardwaj, Jagdish Gohil, Jitendriya Biswal, Nimesh Raj, Lovish Dhingra, V. C. Patil.
Research: Jamuna KV, Uma Bhardwaj, Jagdish Gohil, Jitendriya Biswal, Nimesh Raj, Lovish Dhingra, V. C. Patil.
Methodology: Jamuna KV, Uma Bhardwaj, Jagdish Gohil, Jitendriya Biswal, Nimesh Raj, Lovish Dhingra, V. C. Patil.
Project management: Jamuna KV, Uma Bhardwaj, Jagdish Gohil, Jitendriya Biswal, Nimesh Raj, Lovish Dhingra, V. C. Patil.
Resources: Jamuna KV, Uma Bhardwaj, Jagdish Gohil, Jitendriya Biswal, Nimesh Raj, Lovish Dhingra, V. C. Patil.
Software: Jamuna KV, Uma Bhardwaj, Jagdish Gohil, Jitendriya Biswal, Nimesh Raj, Lovish Dhingra, V. C. Patil.
Supervision: Jamuna KV, Uma Bhardwaj, Jagdish Gohil, Jitendriya Biswal, Nimesh Raj, Lovish Dhingra, V. C. Patil.
Validation: Jamuna KV, Uma Bhardwaj, Jagdish Gohil, Jitendriya Biswal, Nimesh Raj, Lovish Dhingra, V. C. Patil.
Display: Jamuna KV, Uma Bhardwaj, Jagdish Gohil, Jitendriya Biswal, Nimesh Raj, Lovish Dhingra, V. C. Patil.
Drafting - original draft: Jamuna KV, Uma Bhardwaj, Jagdish Gohil, Jitendriya Biswal, Nimesh Raj, Lovish Dhingra, V. C. Patil.
Writing - proofreading and editing: Jamuna KV, Uma Bhardwaj, Jagdish Gohil, Jitendriya Biswal, Nimesh Raj, Lovish Dhingra, V. C. Patil.
ANNEXES
|
Acronyms |
Description |
|
QoL |
Quality of Life |
|
ML |
machine learning |
|
WHO |
World Health Organization |
|
IDH |
Intradialytic hypotension |
|
GFR |
glomerular filtration rate |
|
CKD |
Chronic kidney disease |
|
ESKD |
end-stage kidney disease |
|
irAEs |
immune related adverse events |
|
TIR |
time in range |
|
MQGWO |
mutant quantum grey wolf optimizer |
|
fluffy K-nearest neighbour |
FKNN |
|
CDC |
Centres for Disease Control |
|
DL |
deep learning |
|
RF |
random forest |
|
PEPM |
patient exact payment model |
|
UOP |
urine output |
|
NGAL |
neutrophil gelatinase-related lipocalin levels |
|
NT-proBNP |
N-terminal B-type natriuretic peptide |
|
ESRD |
end-stage renal disease |