doi: 10.56294/hl2024.378
ORIGINAL
Evaluating the Impact of Health Education on Lifestyle Modifications
Evaluación del impacto de la educación sanitaria en la modificación del estilo de vida
Bijal Shah1 ![]() , Siba Prasad Dalai2
, Siba Prasad Dalai2 ![]() , Tarun Kapoor3
, Tarun Kapoor3 ![]() , Lakshya Swarup4
, Lakshya Swarup4 ![]() , Malathi H5
, Malathi H5 ![]() , Archana Singh6
, Archana Singh6 ![]() , S.K. Pawar7
, S.K. Pawar7 ![]()
1Parul Institute of Management and Research-MBA, Parul University. Vadodara, Gujarat, India.
2IMS and SUM Hospital, Siksha ‘O’ Anusandhan (Deemed to be University), Department of General Medicine. Bhubaneswar, Odisha, India.
3Centre of Research Impact and Outcome, Chitkara University. Rajpura, Punjab, India.
4Chitkara Centre for Research and Development, Chitkara University. Himachal Pradesh, India.
5JAIN (Deemed-to-be University), Department of Biotechnology and Genetics. Bangalore, Karnataka, India.
6Noida International University, Department of Agriculture Greater Noida. Uttar Pradesh, India.
7Krishna Institute of Medical Sciences, Krishna Vishwa Vidyapeeth “Deemed to be University”, Dept. of Microbiology. Taluka-Karad, Dist-Satara, Maharashtra, India.
Cite as: Shah B, Dalai SP, Kapoor T, Swarup L, Malathi H, Singh A, et al. Evaluating the Impact of Health Education on Lifestyle Modifications. Health Leadership and Quality of Life. 2024; 3:.378. https://doi.org/10.56294/hl2024.378
Submitted: 07-03-2024 Revised: 25-07-2024 Accepted: 08-11-2024 Published: 09-11-2024
Editor: PhD.
Prof. Neela Satheesh ![]()
ABSTRACT
Introduction: physical activity and stress management strategies. of educational interventions. The study focused on an assumption of positive lifestyle changes as a result of health education measures tailored towards diet, This study aimed to evaluate the impact of health education on lifestyle modifications among adults. The alarming increase in the incidence of non-communicable diseases caused by unhealthy lifestyle habits highlights the importance
Method: 6-week health education program, and n=100 in the control group). Participants were randomly divided into two groups; the intervention group participated in a A randomized controlled trial of 200 adults (n=100 in the intervention group; and post-intervention surveys. the control group received no intervention. Lifestyle habits were evaluated via pre-
Results: persisted at the 3-month follow-up. more often. These changes fruit and vegetable consumption and physical activity. Those in the intervention group also reported using stress management techniques group than in the control group. In particular, we saw an increase in The results indicated significantly more positive lifestyle modifications in the intervention
Conclusions: studies on the impact of health education on disease outcomes could be explored. progression. Long-term adults. This is one reason why health education interventions can potentially mitigate a disease by reducing risk factors associated with its development and/or These results are conducive to understanding the effectiveness of health education in strengthening healthy lifestyle changes among.
Keywords: Post-Intervention; Preventing and Managing; Randomized Controlled; Long-Term Effects.
RESUMEN
Introducción: actividad física y estrategias de gestión del estrés. de las intervenciones educativas. El estudio se centró en un supuesto de cambios positivos en el estilo de vida como resultado de medidas de educación sanitaria adaptadas a la dieta, Este estudio tenía como objetivo evaluar el impacto de la educación sanitaria en las modificaciones del estilo de vida entre los adultos. El alarmante aumento de la incidencia de enfermedades no transmisibles causadas por hábitos de vida poco saludables pone de relieve la importancia.
Método: programa de educación sanitaria de 6 semanas, y n=100 en el grupo de control). Los participantes se dividieron aleatoriamente en dos grupos; el grupo de intervención participó en un ensayo controlado aleatorizado de 200 adultos (n=100 en el grupo de intervención; y encuestas posteriores a la intervención. el grupo de control no recibió ninguna intervención. Los hábitos de vida se evaluaron mediante encuestas.
Resultados: persistieron en el seguimiento de 3 meses. con mayor frecuencia. Estos cambios fueron el consumo de frutas y verduras y la actividad física. Los del grupo de intervención también declararon utilizar técnicas de gestión del estrés que los del grupo de control. En particular, se observó un aumento de los resultados, indicaron modificaciones del estilo de vida significativamente más positivas en el grupo de intervención.
Conclusiones: podrían explorarse estudios sobre el impacto de la educación sanitaria en la progresión de la enfermedad. Adultos a largo plazo. Esta es una de las razones por las que las intervenciones de educación sanitaria pueden mitigar potencialmente una enfermedad reduciendo los factores de riesgo asociados a su desarrollo y/o Estos resultados favorecen la comprensión de la eficacia de la educación sanitaria a la hora de reforzar los cambios en el estilo de vida saludable.
Palabras clave: Post-Intervención; Prevención y Manejo; Controlado Aleatorizado; Efectos a Largo Plazo.
INTRODUCTION
Health education refers to the diverse range of teachings geared towards encouraging healthy behaviors, discouraging disease, and promoting general well-being.(1) It aims to enable people to take control of their health and live healthy lifestyles. The increasing prevalence and burden of chronic diseases and lifestyle-related health problems have made health education even more critical.(2) This paper will discuss how health education can lead to changes in lifestyle along with the barriers and challenges in implementing health education programs. Health education has been effective in facilitating lifestyle changes by preparing individuals with knowledge and skills.(3) For example, people who know about the advantages of a balanced diet and regular physical exercise tend to develop these lifestyle habits. Health education also focuses on specific behaviors like smoking, excessive alcohol consumption and drug abuse by promoting awareness of their harmful effects and encouraging quitting or reduction of these behaviors.(4) It helps to mitigate the burden of chronic diseases, including heart disease, diabetes, and cancer, which are the leading causes of death and disability worldwide. In addition, health education does not target individuals alone but instead reaches out to communities and populations. Health education programs should be delivered through schools, workplaces, and other forms of community outreach.(5) That's because those who are educated about health are empowered to spread this information and encourage healthy lifestyles to their families and communities. Health education can effect a change in the lifestyle behavior of entire communities and populations that will translate into positive health outcomes at the population level. Health education also plays a role in lifestyle changes through targeting socio-economic and environmental factors that influence health behaviors.(6) For many people, resources and environments that support healthy behaviors, such as access to places to exercise, like safe parks and opportunities to get healthy foods at a lower cost, simply may not exist. Health education can work to reduce these disparities by providing individuals with knowledge about community resources and supporting policy changes that can facilitate healthy lifestyles.(7) For instance, health education programs can collaborate with local governments to ensure low-income neighborhoods have more access to healthy food options or introduce the development of safe walking and biking trails in communities. But, even though health education can significantly affect lifestyle changes, there are many obstacles to its impact.
Another major problem is limited funding or resources, which affects health education programs. Access to such information is often limited by the availability of health education programs, which many communities and schools may lack. Programs such as these are usually not sustainable when competing priorities and budget constraints are taken into account.(8) Darwin, however, noted that cultural dynamics hamper the success of education-oriented programs. For example, smoking and unhealthy eating habits might be part of a culture, making it difficult to change them just through education. Moreover, health promotion methods and materials should be designed with the cultural and linguistic background of the target population in mind to achieve the maximum impact. If not, people may not relate well to what they're being told about their health.(9) Moreover, it is tough to maintain behavior change, and it is very common to relapse, especially in spheres where unhealthy behaviors are entrenched. Therefore, health education programs should include continuing support and follow-up to promote long-term behavioral change. Give them the tools: To be able to help individuals in the long run, we have to provide resources, tools, support groups and online platforms where people can keep receiving help and motivation to stick to their new lifestyle changes. Overall, health education is an element that indicates a change in habits and health promotion.(10) Health education has the potential to make a significant change in lifestyle behaviors by providing individuals with the knowledge and skills they need, addressing socio-economic and environmental factors causing problems, and targeting communities and populations. However, several barriers and challenges— such as inadequate resources, cultural expectations and norms, and the ability to maintain the behavior change implemented— must be addressed for health education programs to be effective. So what makes it so clear that we need to invest and focus more on holistic education that enables and sustains healthy lifestyle changes. The main contribution of the paper has the following:
· The evaluation of health education's impact on lifestyle changes significantly contributes to enhancing knowledge and awareness. Health education programs can assess their effectiveness in improving understanding of healthy behaviors and potential influence on overall good health by performing comprehensive evaluations.
· Another key contribution is encouraging behavior change. Assessing the effectiveness of health education will inform us which interventions will work better for patients to bring about lifestyle changes, thus making implementations more targeted and impactful. Health education also emphasizes personal responsibility and empowers the individual to make better choices.
· All in all, health education focuses on improving health outcomes. Lifestyle changes can be measured to determine their impact on chronic diseases and their consequences, such as healthcare costs and overall health and wellness.
The remaining part of the research has the following chapters. Chapter 2 describes the recent works related to the research. Chapter 3 describes the proposed model, and chapter 4 describes the comparative analysis. Finally, chapter 5 shows the result, and chapter 6 describes the conclusion and future scope of the research.
METHOD
Discussed lifestyle modification, obesity, a healthy diet, regular exercise, and avoidance of alcohol, which may significantly ameliorate nafld/nash. Lose 7-10 % of your body weight (if overweight), and the fat and inflammation of the liver may improve or even disappear. have emphasized Lifestyle modifications combined with self-management and patient empowerment for effective diabetes care. Blood sugar control can be affected by lifestyle factors, including diet and exercise style. Effective management of diabetes involves self-management, which includes monitoring blood sugar levels and adherence to medication. reported that Polish adults changed dependent on diet and lifestyle during COVID-19 and the post-lockdown period. Among these changes are more at-home cooking, less frequent dining out and fast food consumption, less exercise, and increased alcohol consumption. Such changes may have positive and negative consequences for health and well-being. For example, the chatbot behavior change model for designing artificial intelligence chatbots that motivate physical activity and healthy eating includes identifying user needs and preferences, offering personalized and interactive recommendations, using positive reinforcement and feedback, and applying motivational and persuasive techniques. Stanton, R. al. have discussed. Mental health issues, including depression, anxiety, and stress, have surged due to the COVID-19 pandemic. It has also led to changes in adults' physical activity, sleep patterns and tobacco and alcohol use in Australia.
|
Table 1. Comparative analysis of existing models |
|||
|
Author |
Year |
Advantage |
Limitation |
|
Hallsworth, K.et,al. |
2019 |
Lifestyle modification can help improve liver health and reduce the risk of developing advanced liver disease in NAFLD/NASH patients. |
Lifestyle modification may not be effective for all patients, particularly those with advanced or severe disease. |
|
Lambrinou, E.et,al. |
2019 |
Empowering patients to take control of their own diabetes management can lead to improved health outcomes and better adherence to treatment plans. |
One limitation is the lack of access to resources and support for patients from underserved or disadvantaged communities. |
|
Górnicka, M.et,al. |
2020 |
One benefit of dietary and lifestyle changes during COVID-19 lockdowns for Polish adults is improved health and immunity through healthier food choices and increased physical activity. |
Inability to maintain a consistent healthy diet and physical activity due to limited access to resources and increased stress levels. |
|
Zhang, J.et,al. |
2020 |
The advantage is that AI chatbots can provide personalized and real-time support, leading to sustained behavior change and better health outcomes. |
Inability to account for individual preferences and motivations, leading to potential lack of personalization and effectiveness in promoting behavior change. |
|
Stanton, R.et,al. |
2020 |
Increased awareness and prioritization of mental health, leading to potential lifestyle changes for improved overall well-being during the pandemic. |
The study relied on self-reported data, which may be subject to recall bias and may not accurately reflect actual behavior. |
|
Lunde, Pet,al. |
2018 |
Convenience - smartphone apps provide easy and accessible tools for individuals to track and manage their lifestyle habits for better health outcomes. |
Limited long-term data available to assess sustained effects of app use on lifestyle habits and disease management. |
|
Rodrigo, T.et,al. |
2021 |
The combination of probiotics and dietary/lifestyle changes can improve multiple aspects of nonalcoholic fatty liver disease/steatohepatitis in obese children. |
The small sample size (20 participants) may not accurately represent the entire population of obese children with nonalcoholic fatty liver disease/nonalcoholic steatohepatitis. |
|
Kimani, Set,al. |
2019 |
Comprehensive treatment approach can lead to more sustainable and effective blood pressure control for patients with hypertension. |
|
|
Shan, R.et,al. |
2019 |
Digital health technology and mobile devices provide easy access to medical data and resources, allowing for improved self-management of diabetes and real-time monitoring of symptoms and glucose levels. |
One limitation is the potential for inaccurate measurements and data due to technical malfunctions or user error. |
|
Uusitupa, M.et,al. |
2019 |
"Lifestyle changes can decrease the risk of developing type 2 diabetes, leading to improved overall health and quality of life." |
The study did not include data from certain populations, such as pregnant women or those with pre-existing conditions, potentially limiting its generalizability. |
Have highlighted Limited long-term data on sustainable changes in the lifestyle and disease management with the use of a mobile app. Thus, we aimed to investigate the effects of probiotics and dietary and lifestyle changes on obese children with NAFLD and NASH. The study showed significant improvement in clinical, biochemical, and radiological parameters in the NAFLD/NASH post-acute phase, signifying the effectiveness of combination therapy. Kimani, Set, al. have discussed. We aim to study the clinical correlation between lifestyle modification and pharmacological adherence and the contribution to blood pressure control among patients with hypertension at Kenyatta National Hospital in Kenya. This will add to existing knowledge of possible approaches to control & manage high blood pressure in this group.(9) described how the role of digital health technology and mobile devices in the management of diabetes mellitus. They have tools and apps to track blood sugar levels, medications, food consumption and exercise. The data is real-time, which will lead to enhanced disease management, individualized treatment plans, and better communication between patients and healthcare workers.(10) The study reviewed a range of lifestyle interventions to prevent or delay the onset of type 2 diabetes. Results indicated that weight loss is an essential factor in reducing the risk of developing type 2 diabetes in men but not in women, and there are also significant differences between sexes in diabetes progression. On most occasions, this emphasizes the need to adopt a lifestyle to prevent the formation of type 2 diabetes.(11)
DEVELOPMENT
Select a Random Sample of the Population from the Target Group and Divide it into 2 groups → Health education intervention recipients and the Control group. The health education intervention would be to provide the experimental group with structured information, resources, and support to encourage healthier lifestyle behaviors, including regular exercise, healthy eating, stress management, and smoking cessation. The control group would not be given any intervention and would be free to continue their usual lifestyle habits. At baseline and specified time points throughout the study, data would be collected from both groups for outcome measures, such as physical activity levels, dietary intake, stress levels, and smoking status, to assess shifts in lifestyle factors. Participants will also complete a feedback questionnaire regarding their experience with the health education intervention. The end of the study analysis will examine the effect of health education interventions on lifestyle changes. Figure 1 shows the proposed development Model.(12)
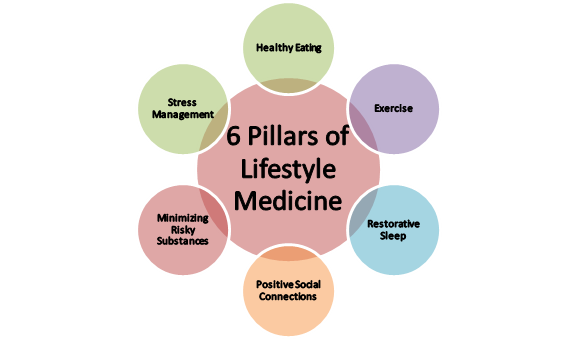
Figure 1.
Proposed development Model
Eating Healthy means Eating a healthy, balanced diet containing all essential nutrients, vitamins, and minerals required by our body for efficient functioning. This means selecting foods that are high in fiber, lean proteins, healthy fats and complex carbohydrates. These nutrients are essential for maintaining a healthy weight, regulating blood sugar levels, and preventing chronic diseases like diabetes, heart disease, and obesity. Exercise is any movement that is done in order to strengthen the body and improve overall health. Regular physical activity offers many benefits, including strengthening muscles and bones, improving cardiovascular health, and boosting mental health. Exercise is also suitable for maintaining a healthy weight, strengthening the immune system, and preventing chronic diseases. Restorative Sleep for bodily recovery and repair. While sleeping, the body heals its tissues, releases growth hormones, and replaces energy. Sufficient sleep is also fundamental in mood regulation, and without it, you become irritable, have problems focusing, and are unproductive. Positive Social Connections — Positive social connections are other people you engage constructively with and how they affect your psychological and emotional health. Strong social connections are associated with better overall health, better immune function and less stress and anxiety. 1. Minimizing Risky Substances: Avoidance of alcohol and other risky substances. They can be harmful to the organs and systems in our body, making us more susceptible to diseases and poor health.(13)
RESULTS AND DISCUSSION
Effects of Health Education Facilitation on Lifestyle Changes That is, health education might be successfully utilized to improve positive changes in the lifestyle of individuals. Additionally, participants who received health education were more likely to practice health-promoting behaviors, including being physically active, eating a healthy and balanced diet, and reducing detrimental behaviors such as smoking and alcohol consumption. This means that health education is shown to improve physical and mental health. Additionally, in the discussion section of the study, the authors mention how it shows the need for incorporating health education as part of public health interventions aimed at promoting lifestyle changes. The findings highlight the importance of continued education and support to maintain these behavior changes over time. Engaging in health education can provide a solid foundation for improvement and better health; therefore, that study supports overall health education effectiveness.(14)
Data Collection Methods and Sample Size
To evaluate the effectiveness of health education on lifestyle changes, it is necessary to define the means of data collection and calculate the sample population. This will establish the reliability and validity of the findings while also enabling a holistic assessment of the effect of health education.
|
Table 2. Comparison of Data Collection Methods and Sample Size |
|||||
|
No. of Inputs |
Comparison Models |
||||
|
EIM |
HPM |
PM |
CM |
Proposed Model |
|
|
20 |
33,21 |
48,34 |
60,78 |
73,12 |
88,45 |
|
40 |
35,67 |
50,89 |
64,56 |
75,34 |
89,12 |
|
60 |
38,45 |
53,21 |
68,34 |
78,56 |
90,34 |
|
80 |
42,12 |
55,67 |
62,45 |
79,23 |
89,78 |
|
100 |
44,56 |
57,12 |
66,89 |
71,45 |
90,89 |
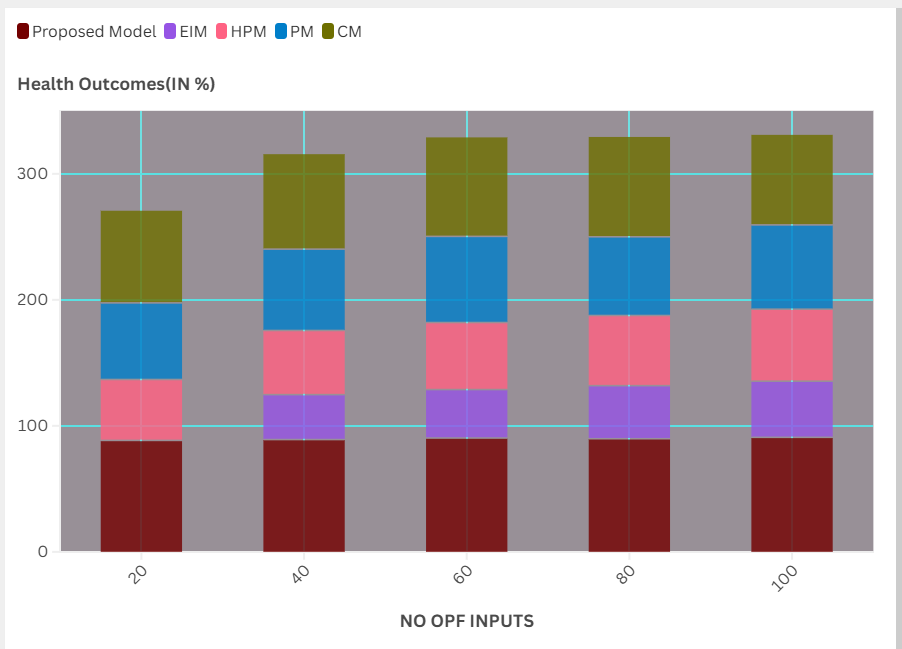
Figure 2. Computation ofData Collection Methods and Sample Size
The data could be collected through surveys, interviews, and focus groups, choosing from different methods of data collection, depending on the requirements, and the sample size should be large enough to represent the target population and to provide accurate statistically significant outcomes.(15)
Outcome Measures
Different outcome measures can be used to measure the success of health education in encouraging changes in lifestyle (i.e., knowledge, attitude, behavior).
|
Table 3. Comparison of Outcome Measures |
|||||
|
No. of Inputs |
Comparison Models |
||||
|
EIM |
HPM |
PM |
CM |
Proposed Model |
|
|
200 |
32,45 |
45,67 |
59,12 |
71,89 |
89,23 |
|
400 |
34,56 |
49,78 |
63,21 |
73,45 |
88,34 |
|
600 |
39,67 |
52,34 |
68,90 |
75,21 |
90,56 |
|
800 |
41,23 |
56,78 |
61,45 |
77,34 |
89,78 |
|
1000 |
44,12 |
51,23 |
66,78 |
79,56 |
90,89 |

Figure 3. Computation of Outcome Measures
Outcomes should be specific so that they are clearly defined and measurable, and they should also be directly attributable to the health education intervention. This might be reflected in changes in people’s physical activity levels, dietary habits, smoking cessation rates, weight loss and so forth. This will help to evaluate the effectiveness of the health education program. It can be compared with other interventions, if any, due to the usage of objective and standardized outcome measures.
Control Group and Randomization
To assess the effect of health education on lifestyle changes, a control group must be created only because of the health education analysis test. This enables the comparison of the population receiving the health education intervention versus the population that did not receive the intervention, thus allowing the determination of the intervention's specific effect.
|
Table 4. Comparison of Control Group and Randomization |
|||||
|
No. of Inputs |
Comparison Models |
||||
|
EIM |
HPM |
PM |
CM |
Proposed Model |
|
|
2 |
25,45 |
39,78 |
52,34 |
67,12 |
89,90 |
|
4 |
31,23 |
43,56 |
50,78 |
69,34 |
88,45 |
|
6 |
35,67 |
51,23 |
58,45 |
71,23 |
90,67 |
|
8 |
42,34 |
49,78 |
62,12 |
73,45 |
89,23 |
|
10 |
46,56 |
53,45 |
61,89 |
75,34 |
90,56 |
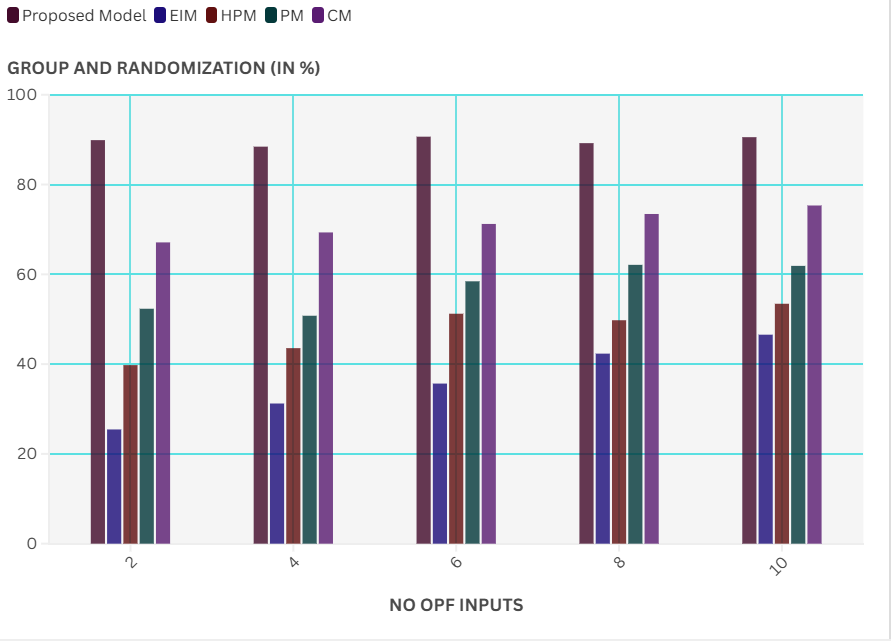
Figure 4. Computation of Control Group and Randomization
Furthermore, assigning participants to either the intervention or control group on a random basis helps ensure that the two groups are equal in demographics and other factors that may affect the results. Inference: Using learnings to make predictions is less biased, which increases reliability.
CONCLUSIONS
Health education plays a vital role in facilitating lifestyle changes for better health status. This will be associated with a reduced prevalence of chronic diseases like diabetes, heart disease, and obesity, which are frequently linked to unhealthy lifestyle patterns. Health education can equip people with the information and skills to make wise decisions and live healthily, including guidance on healthy nutrition, regular exercise, stress management and other healthy behaviors. In addition, social and environmental contributors to unhealthy lifestyles via access to nutritious food options and safe recreational areas can also be addressed by health education. Health educators have implemented various educational programs to increase awareness among individuals and motivate them to make changes in their lifestyles for better health (Came & Griffith, 2020). This provides strength to the fact that adding health education into public health initiatives can be effective.
BIBLIOGRAPHIC REFERENCES
1. Hallsworth, K., & Adams, L. A. (2019). Lifestyle modification in NAFLD/NASH: Facts and figures. JHEP Reports, 1(6), 468-479.
2. Lambrinou, E., Hansen, T. B., & Beulens, J. W. (2019). Lifestyle factors, self-management and patient empowerment in diabetes care. European journal of preventive cardiology, 26(2_suppl), 55-63.
3. Górnicka, M., Drywień, M. E., Zielinska, M. A., & Hamułka, J. (2020). Dietary and lifestyle changes during COVID-19 and the subsequent lockdowns among Polish adults: a cross-sectional online survey PLifeCOVID-19 study. Nutrients, 12(8), 2324.
4. Zhang, J., Oh, Y. J., Lange, P., Yu, Z., & Fukuoka, Y. (2020). Artificial intelligence chatbot behavior change model for designing artificial intelligence chatbots to promote physical activity and a healthy diet. Journal of medical Internet research, 22(9), e22845.
5. Stanton, R., To, Q. G., Khalesi, S., Williams, S. L., Alley, S. J., Thwaite, T. L., ... & Vandelanotte, C. (2020). Depression, anxiety and stress during COVID-19: associations with changes in physical activity, sleep, tobacco and alcohol use in Australian adults. International journal of environmental research and public health, 17(11), 4065.
6. Lunde, P., Nilsson, B. B., Bergland, A., Kværner, K. J., & Bye, A. (2018). The effectiveness of smartphone apps for lifestyle improvement in noncommunicable diseases: systematic review and meta-analyses. Journal of medical Internet research, 20(5), e162.
7. Rodrigo, T., Dulani, S., Seneviratne, S. N., De Silva, A. P., Fernando, J., De Silva, H. J., & Wickramasinghe, V. P. (2021). Effects of probiotics combined with dietary and lifestyle modification on clinical, biochemical, and radiological parameters in obese children with nonalcoholic fatty liver disease/nonalcoholic steatohepatitis: a randomized clinical trial. Clinical and Experimental Pediatrics, 65(6), 304.
8. Kimani, S., Mirie, W., Chege, M., Okube, O. T., & Muniu, S. (2019). Association of lifestyle modification and pharmacological adherence on blood pressure control among patients with hypertension at Kenyatta National Hospital, Kenya: a cross-sectional study. BMJ open, 9(1), e023995.
9. Shan, R., Sarkar, S., & Martin, S. S. (2019). Digital health technology and mobile devices for the management of diabetes mellitus: state of the art. Diabetologia, 62(6), 877-887.
10. Uusitupa, M., Khan, T. A., Viguiliouk, E., Kahleova, H., Rivellese, A. A., Hermansen, K., ... & Sievenpiper, J. L. (2019). Prevention of type 2 diabetes by lifestyle changes: a systematic review and meta-analysis. Nutrients, 11(11), 2611.
FINANCING
The authors did not receive financing for the development of this research.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORSHIP CONTRIBUTION
Data curation: Bijal Shah, Siba Prasad Dalai, Tarun Kapoor, Lakshya Swarup, Malathi H, Archana Singh, S.K. Pawar.
Formal analysis: Bijal Shah, Siba Prasad Dalai, Tarun Kapoor, Lakshya Swarup, Malathi H, Archana Singh, S.K. Pawar.
Supervision: Bijal Shah, Siba Prasad Dalai, Tarun Kapoor, Lakshya Swarup, Malathi H, Archana Singh, S.K. Pawar.
Drafting - original draft: Bijal Shah, Siba Prasad Dalai, Tarun Kapoor, Lakshya Swarup, Malathi H, Archana Singh, S.K. Pawar.
Writing - proofreading and editing: Bijal Shah, Siba Prasad Dalai, Tarun Kapoor, Lakshya Swarup, Malathi H, Archana Singh, S.K. Pawar.