doi: 10.56294/hl2022133
ORIGINAL
Advancing Healthcare Competence in the Management of Rheumatic Heart Disease in Primary Healthcare Settings
Fomento de la competencia sanitaria en el tratamiento de la cardiopatía reumática en los centros de atención primaria
Ram
Garg1 ![]() , Wakeel Ahmed2
, Wakeel Ahmed2
![]() , Deepak Kumar Parhi3
, Deepak Kumar Parhi3
![]()
1Arya College of Pharmacy. Jaipur, India.
2Noida International University, School of Liberal Arts. Greater Noida, India.
3IMS and SUM Hospital, Siksha ‘O’ Anusandhan (Deemed to be University), Department of Cardiology. Bhubaneswar, India.
Cite as: Garg R, Ahmed W, Parhi DK. Advancing Healthcare Competence in the Management of Rheumatic Heart Disease in Primary Healthcare Settings. Health Leadership and Quality of Life. 2022; 1:133. https://doi.org/10.56294/hl2022133
Submitted: 13-08-2022 Revised: 31-10-2022 Accepted: 15-12-2022 Published: 16-12-2022
Editor:
PhD. Prof. Neela Satheesh ![]()
ABSTRACT
Rheumatic Heart Disease (RHD) remains a significant global health issue, particularly in primary healthcare settings. Enhancing healthcare competence in RHD management was crucial for early detection and effective treatment. The investigation aims to improve healthcare workers’ competence in managing RHD through targeted training programs and assess the impact on their knowledge and clinical practices. Pre- and post-training surveys were used to assess knowledge, confidence, and practices. Clinical observations were conducted in 46 primary healthcare settings, involving 94 healthcare workers. Variables include knowledge level, Confidence in RHD Management, clinical practice adherence, diagnostic accuracy, and patient education effectiveness. Statistical analysis using SPSS Version 25, including the Paired t-test and Wilcoxon Signed-Rank Test showed significant improvements in healthcare workers’ competence in RHD diagnosis, treatment, and patient education (p<0,05). The Paired t-test was used to compare the mean differences in pre- and post-training scores for normally distributed data, it helps determine whether the mean difference between the two sets of data was statistically significant. The Wilcoxon Signed-Rank Test assessed if there was significant variation between the two related samples (before and after training) by looking at the rank order of the differences rather than the actual values. The training program effectively enhanced healthcare workers’ competence in managing RHD. The intervention holds promise for improving RHD outcomes in primary healthcare settings, with potential for broader implementation.
Keywords: Healthcare; Rheumatic Heart Disease (RHD); Paired t-Test; Wilcoxon Signed-Rank Test; Management.
RESUMEN
La cardiopatía reumática sigue siendo un importante problema de salud mundial, sobre todo en los centros de atención primaria. La mejora de la competencia del personal sanitario en el manejo de la EAR es crucial para la detección precoz y el tratamiento eficaz. El objetivo de esta investigación es mejorar la competencia de los profesionales sanitarios en el tratamiento de la cardiopatía reumática mediante programas de formación específicos y evaluar el impacto en sus conocimientos y prácticas clínicas. Se utilizaron encuestas previas y posteriores a la formación para evaluar los conocimientos, la confianza y las prácticas. Se realizaron observaciones clínicas en 46 centros de atención primaria, con la participación de 94 profesionales sanitarios. Las variables incluyen el nivel de conocimientos, la confianza en el manejo de la EHR, la adherencia a la práctica clínica, la precisión diagnóstica y la eficacia de la educación del paciente. El análisis estadístico realizado con el programa SPSS versión 25, incluida la prueba de la t emparejada y la prueba de rangos con signo de Wilcoxon, mostró mejoras significativas en la competencia de los profesionales sanitarios para el diagnóstico, el tratamiento y la educación de los pacientes con EHR (p<0,05). La prueba t emparejada se utilizó para comparar las diferencias medias en las puntuaciones previas y posteriores a la formación para datos distribuidos normalmente, y ayuda a determinar si la diferencia media entre los dos conjuntos de datos era estadísticamente significativa. La prueba de rangos con signo de Wilcoxon evaluó si existía una variación significativa entre las dos muestras relacionadas (antes y después de la formación) fijándose en el orden de rango de las diferencias en lugar de en los valores reales. El programa de formación mejoró eficazmente la competencia del personal sanitario en el manejo de la EHR. Se trata de una intervención prometedora para mejorar los resultados de la enfermedad en los centros de atención primaria, con potencial para una aplicación más amplia.
Palabras clave: Atención Sanitaria; Cardiopatía Reumática; Prueba t Pareada; Prueba de Rangos con Signo de Wilcoxon; Tratamiento.
INTRODUCTION
The influence of Rheumatic Heart Disease (RHD) on the illnessproblem of afflicted peoples makes it a significant source of cardiovascular illness and mortality in several developing countries.(1) RHD is a long-term complication of Rheumatic Fever (RF), which typically follows untreated or inadequately treated streptococcal throat infections.(2) Primary healthcare (PHC) centers for the affected population are the centers where people can first report their symptoms related to RHD, which assigns great importance to the anticipation, early analysis, and further administration of the disease in these centers. Effective early diagnosis and intervention in PHC could help avoid the advance of RF to RHD saving more costs and invasive corrective procedures such as valve replacement surgery.(3) Furthermore, the management of RHD in PHC involves a multidisciplinary approach, including the use of antibiotics for secondary prophylaxis, regular monitoring, and patient education to prevent recurrent infections.(4) However, treating RHD in PHC settings is fraught with difficulties.Early identification and prompt treatment of RHD are hampered by a lack of diagnostic instruments in many PHC facilities, insufficient funding, and poor provider training.(5) In addition, RHD is frequently not well understood by the general public and medical professionals, which causes delays in diagnosis and treatment.(6) A large number of patients with various health conditions overwhelms healthcare systems in some areas, taking focus away from RHD care. Compounding the issue is the lack of established referral networks between PHC and secondary or tertiary care, which restricts access to specialized treatment.(7) Furthermore, economic constraints in PHC settings result in the underutilization of available resources, which limits the implementation of effective prevention strategies. The lack of comprehensive data and monitoring systems to track the prevalence and progress of RHD also impedes long-term planning for its control. Structural barriers such as inadequate infrastructure and healthcare workforce shortages also contribute to delays in care delivery.(8) This research aims to assess the impact of targeted training programs on the clinical practices and knowledge of healthcare professionals while improving their ability to manage RHD.
Related works
The research evaluated the current level of healthcare linked to RHD, including insufficient information, diagnostic procedure deficiencies, and pharmaceutical supply constraints. The absence of diagnostic testing, unclear rules, and low district-level understanding were among the obstacles to supplying RHD-related treatment. It also suggested improving the distribution systems including diagnoses and needed medications, decentralized RHD diagnosis and detection, and providing specialist instruction.(9) The effects of RHD worldwide looking at a wide variety of issues such as illness burden, the effect on the healthcare system, and socioeconomic ramifications. The treatable illness has a detrimental impact on individuals, as well as the communities and healthcare systems in which they reside. The process of avoidance, detection, and treatment was filled with difficulties and expensive.(10 )The investigation suggested multisectoral cooperation to address the impact of RHD by involving the public, medical professionals, and legislators, enhancing healthcare support. It also improved prophylactic distribution methods and raised technological advancement and research as vital interventions to spare millions of people from avoidable morbidity and mortality.(11) The investigation examined care models for pregnant women with RHD from the viewpoint of medical professionals. Healthcare systems, workers, and subcultures are some of the variables that make providing holistic women-centered care difficult. Treatment conductors, layers, and mutual comprehension are concepts that impact the caliber of care. These elements assisted in addressing the difficulty, dismantling data barriers, and enhancing knowledge of diseases and well-informed decision-making.(12) To lead traditional capabilities and employ a critical reflexive attitude to analyze systems, organizations, and procedures, it was essential to integrate physiological and sociological techniques in research, training, and practice. That method improved medical results by fostering fruitful cross-cultural communication and societal change, giving clinicians optimism and orientation, and increasing their ability.(13) The purpose of the research was to examine the Patient-Centered Care (PCC) methods employed by medical staff at a hospital-based Rheumatology Clinic (RC), their relationship to digital technologies, and the alleged impact of these tactics on patients and medical professionals. The significance of psychological and cultural transformation was evident, and the roles of healthcare providers and patients were impacted.(14) The research examined women who had previously been diagnosed with RHD, detailing the clinical and echocardiographic results, finding obstacles to following their prescribed treatment, and assessing the effects of RHD on their individual lives. Pregnancy-related RHD diagnosis could have long-term clinical and psychological effects.(15) Using a paradigm that addressed six domains such as housing and ecological assistance, public engagement and autonomy, medical knowledge, education and medical facility cooperation, medical directions, and healthcare professional education, the research attempted to promote RHD fundamental and preventive measures. Finding out how research participants perceived the model is the purpose. Though that was constrained by the complexity of the condition, it increased health education and promoted understanding and independence.(16)
METHOD
This methodology evaluates the effectiveness of training in enhancing the competency of the healthcare workers in the management of RHD. Demographic data were obtained while statistical analyses were used to assess changes in the levels of healthcare workers’ competence about selected aspects of RHD management.
Data Collection
The investigation’s data collection approach included acquiring demographic information from 94 healthcare professionals in 46 primary care settings. Table 1 depicts the demographic characteristics of healthcare workers. Participants were categorized by gender, age group, years of experience, professional role, region, and healthcare center type. These data were collected to describe the healthcare workers participating in the analysis to assess features that could moderate the effects of the training program on the management of RHD competence.
|
Table 1. Healthcare Workers' Demographic Profile |
|||
|
Variable |
Categories |
Frequency (n) |
Proportion (%) |
|
Sex |
Male |
42 |
44,7 |
|
Female |
52 |
55,3 |
|
|
Age |
20–29 |
18 |
19,1 |
|
30–39 |
35 |
37,2 |
|
|
40–49 |
26 |
27,7 |
|
|
50 and above |
15 |
16,0 |
|
|
Years of Experience |
< 1 year |
5 |
5,3 |
|
1–5 years |
27 |
28,7 |
|
|
6–10 years |
33 |
35,1 |
|
|
> 10 years |
29 |
30,9 |
|
|
Professional Role |
General Practitioner |
36 |
38,3 |
|
Nurse |
42 |
44,7 |
|
|
Other Healthcare Workers |
16 |
17,0 |
|
|
Region |
Urban |
55 |
58,5 |
|
Rural |
39 |
41,5 |
|
|
Healthcare Center Type |
Primary Healthcare Center |
46 |
48,9 |
|
Specialized Healthcare Center |
48 |
51,1 |
|
Selection Criteria
The selection criteria included factors for both inclusion and exclusion to ensure participants were suitable for the analysis, with the inclusion criteria being based on the participant’s experience, and their readiness to contribute in the research, and the exclusion criteria excluded participants, who did not meet the necessary professional qualifications or were unable to participate in the assessments. Table 2 shows the selection criteria process.
|
Table 2. Participants Eligibility Process |
|
|
Inclusion Criteria |
Exclusion Criteria |
|
Healthcare workers employed in primary healthcare settings. |
Healthcare workers are not involved in RHD management or diagnosis. |
|
Must have direct involvement in managing or diagnosing RHD. |
Healthcare workers with less than 6 months of experience in RHD care. |
|
Willingness to participate in pre-and post-training surveys. |
Workers are unable to complete the pre- or post-training surveys. |
Variables
The variables in this research are Knowledge levels which are measured by the pre- and post-training knowledge questionnaires. Self-efficacy of RHD management is assessed using confidence ratings before and after the training. Clinical practice adherence measures the extent to which diagnostic as well as treatment guidelines are followed. Diagnostic accuracy in RHD means the degree to which clinicians make accurate diagnoses of RHD. Patient education effectiveness is measured by the ability of the information being given to patients on RHD issues.
Statistical Analysis
Data were analyzed using the SPSS Version 25 to assess change in healthcare workers’ competence in managing RHD before and after training. Paired t-test was used in measuring normally distributed data about normally distributed services, to establish the significance of the difference between means, before and after training. Further, to determine the significance of differences between the related samples (before and after training), to compare the rank order of the discrepancies, the Wilcoxon signed-rank test was utilized. The actual impact of the training program on the results was evaluated by controlling all possible confounding variables, such as years of experience or professional function, using Analysis of Covariance (ANCOVA). With a p-value of less than 0,05, all tests demonstrated substantial gains in the knowledge, confidence, clinical practice adherence, diagnostic accuracy, and efficacy of patient education of healthcare personnel. This demonstrated the efficacy of the training intervention.
RESULTS
Statistical comparison also shows that the values of the assessed variables have improved after the intervention. Several tests, including paired t-test, Wilcoxon signed-rank test, and ANCOVA analysis further support the training in improving the participants’ knowledge, skills, and confidence, with strong effect sizes and statistical significance across all measures.
Pre- and Post-Training Assessment of Healthcare Worker RHD Competence
Following a focused training program, Table 3 shows a notable increase in healthcare personnel’s proficiency in handling RHD. Pre-test scores ranged from 17 % to 43 %, indicating a lack of understanding in important areas such as early indicators of RF, diagnostic standards, and management techniques. Nonetheless, post-test results showed significant improvements, with 72 % to 96 % of correct responses across a range of subjects, such as screening, diagnostic techniques, and preventative measures. Improvements in areas including identifying RF symptoms, comprehending the diagnostic value of echocardiography, and treating penicillin allergies were the most noticeable. With statistically significant p-values (<0,001), these findings demonstrate how well the training improved the knowledge, abilities, and confidence of healthcare professionals in managing RHD. They also highlight the potential for such programs to improve patient outcomes and advance RHD management in primary healthcare settings.
|
Table 3. Participants’ Responses on Advancing Healthcare Competence in RHD Management |
||||
|
Assessment Area |
Specific Question |
Pre-Test (n, %) |
Post-Test (n, %) |
P-Value |
|
Participants with Correct Answers |
||||
|
Screening and Identification |
What are the early clinical signs of RF in children? |
35 (37 %) |
72 (77 %) |
<0,001 |
|
Which demographic is most at risk for developing RHD? |
40 (43 %) |
80 (85 %) |
<0,001 |
|
|
What is the recommended frequency for screening individuals in high-prevalence areas? |
20 (21 %) |
66 (70 %) |
<0,001 |
|
|
Diagnostic Approaches |
What are the major criteria in the revised Jones criteria for diagnosing RF? |
25 (27 %) |
82 (87 %) |
<0,001 |
|
How is echocardiography utilized to confirm a diagnosis of RHD? |
30 (32 %) |
74 (79 %) |
<0,001 |
|
|
Which laboratory tests are critical for diagnosing recent GAS infections? |
22 (23 %) |
60 (64 %) |
<0,001 |
|
|
Management Strategies |
What is the primary goal of secondary prophylaxis in RF patients? |
55 (59 %) |
90 (96 %) |
<0,001 |
|
Which medications are most effective for treating acute RF symptoms? |
35 (37 %) |
80 (85 %) |
<0,001 |
|
|
How should healthcare workers address penicillin allergies when treating RF? |
38 (40 %) |
82 (87 %) |
<0,001 |
|
|
Prevention and Education |
How can community awareness campaigns help reduce the incidence of RF/RHD? |
20 (21 %) |
66 (70 %) |
<0,001 |
|
What role does vaccination play in preventing streptococcal infections? |
25 (27 %) |
68 (72 %) |
<0,001 |
|
|
What is the impact of timely antibiotic treatment for GAS infections on RF prevention? |
30 (32 %) |
75 (80 %) |
<0,001 |
|
|
Long-Term Outcomes and Digital Tools |
What are the long-term complications of untreated RHD? |
25 (27 %) |
65 (69 %) |
<0,001 |
|
How can digital tools assist healthcare workers in tracking RF/RHD cases? |
16 (17 %) |
58 (62 %) |
<0,001 |
|
|
How does the healthcare infrastructure impact the effectiveness of RHD management programs? |
30 (32 %) |
70 (74 %) |
<0,001 |
|
To determine if the zero and mean discrepancies between two sets of data are significance levels, the mean values of two groups that is associated. This procedure was applied to analyze the before and after test scores from each variable shown in table 4. To compare pre-test and post-test designs before and after the implementation of the program, and to calculate the mean difference, p-value, df, and t-statistic value. The p-values for each of the following variables such as Knowledge Level, Clinical Practice Adherence, Diagnostic Accuracy, Confidence in RHD Management, and Patient Education Effectiveness are stated as <0,001. Therefore, the variances between the before and after test are statistically substantial with extremely high confidence (more than 99,9 %), and the results after the test are for every variable considerably higher than the the prior test scores. Thus, with the largest mean difference (23,5) among the variables, results from Patient Education Effectiveness have been found. Knowledge Level ranks second with a mean difference of 23,3. Both variables exhibited statistically significant increases.
|
Table 4. Outcomes of the paired t-test for the before- and after-test |
||||||||
|
Variable |
Pre-test |
Post-test |
Mean Difference |
t-statistic |
df |
p-value |
||
|
Mean |
SD |
Mean |
SD |
|||||
|
Knowledge Level |
45,2 |
10,5 |
68,5 |
7,8 |
23,3 |
14,1 |
93 |
<0,001 |
|
Confidence in RHD Management |
52,1 |
11,2 |
74,3 |
8,4 |
22,2 |
12,6 |
93 |
<0,001 |
|
Clinical Practice Adherence |
47,8 |
9,4 |
70,0 |
7,5 |
22,2 |
13,8 |
93 |
<0,001 |
|
Diagnostic Accuracy |
50,5 |
10,1 |
72,1 |
8,0 |
21,6 |
12,3 |
93 |
<0,001 |
|
Patient Education Effectiveness |
48,0 |
9,8 |
71,5 |
7,9 |
23,5 |
14,4 |
93 |
<0,001 |
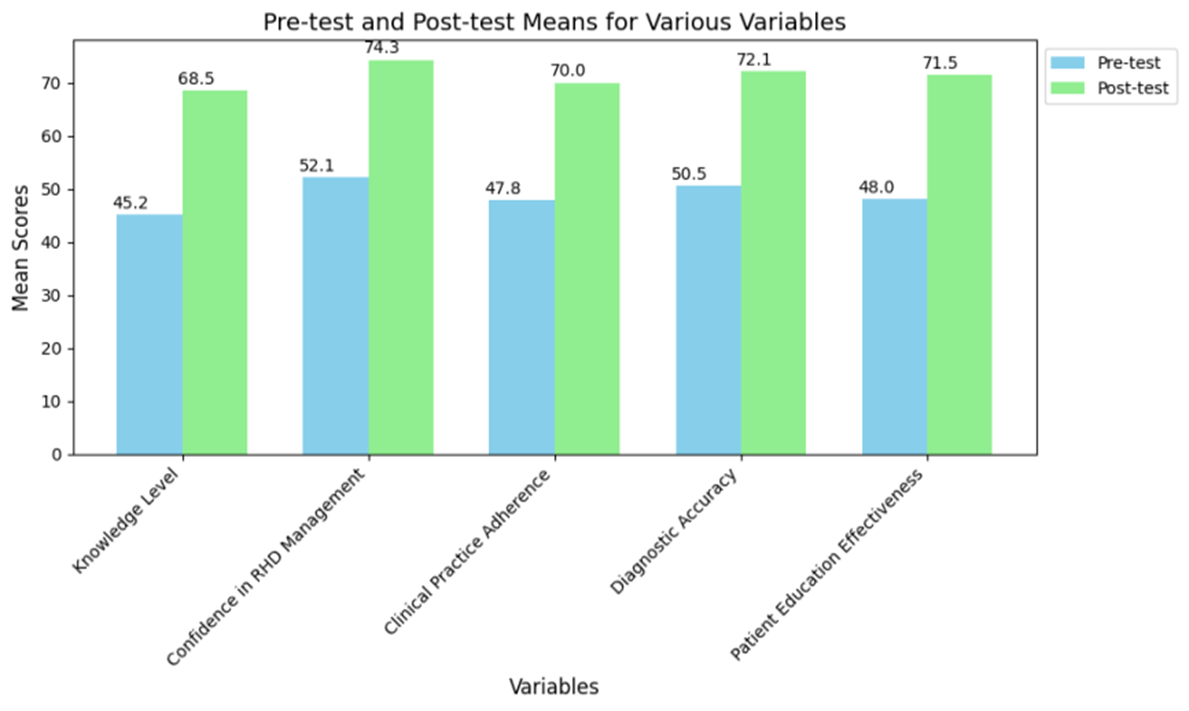
Figure 1. Mean Comparison of various variables
Wilcoxon Signed-Rank Testis also known as the signed-rank test and is used in comparing paired data which is unsuccessful in the normality test, but where the paired t-test cannot be used. Table 5 shows the outcome of the Wilcoxon signed-rank test. By concentrating on the rankings of the differences rather than the actual scores, this test specifically examined two concurrent groups to ascertain whether there is a statistically significant variance in the mean of the differences. It’s most appropriate when using ordinal data or when the distribution of differences is positively skewed. The findings also show that there are changes in all the assessed factors, and the p-values are less than 0,001. This can be concluded from the fact that the mean after training score is significantly higher than the mean before training score on all factors. Results denote the signature strength of medium to large effect size, which for bootstrapped estimates ranges between 0,60 and 0,64. These values demonstrate the training intervention is significant and socially significant in terms of larger effect sizes. Examining these by Z-statistic, Patient Education Effectiveness had the largest negative Z-statistic (-6,22) and measures the largest improvement (ES = 0,64). The remaining variables such as Knowledge Level, Confidence in RHD Management, Clinical Practice Adherence, and Diagnostic Accuracy also depicted increased improvement with effect size over 0,60. The results therefore show the benefits of the training program in enhancing the important competencies and knowledge domains. The strong effect sizes and significant p-values enhance clinical practices and patient-related outcomes. The results presented in this analysis reveal the extensive changes produced by the intervention within all views considered in the assessment.
|
Table 5. Outcomes of the initial and after training variables' Wilcoxon Signed-Rank tests |
|||||
|
Variable |
Pre-training Median (M, SD) |
Post-training Median (M, SD) |
Z-Statistic |
p-value |
Effect Size (r) |
|
Knowledge Level |
45,0 (10,5) |
68,0 (7,8) |
-6,12 |
<0,001 |
0,63 |
|
Confidence in RHD Management |
50,0 (11,2) |
73,0 (8,4) |
-5,85 |
<0,001 |
0,60 |
|
Clinical Practice Adherence |
48,0 (9,4) |
70,0 (7,5) |
-6,01 |
<0,001 |
0,62 |
|
Diagnostic Accuracy |
51,0 (10,1) |
72,0 (8,0) |
-5,95 |
<0,001 |
0,61 |
|
Patient Education Effectiveness |
47,0 (9,8) |
71,0 (7,9) |
-6,22 |
<0,001 |
0,64 |
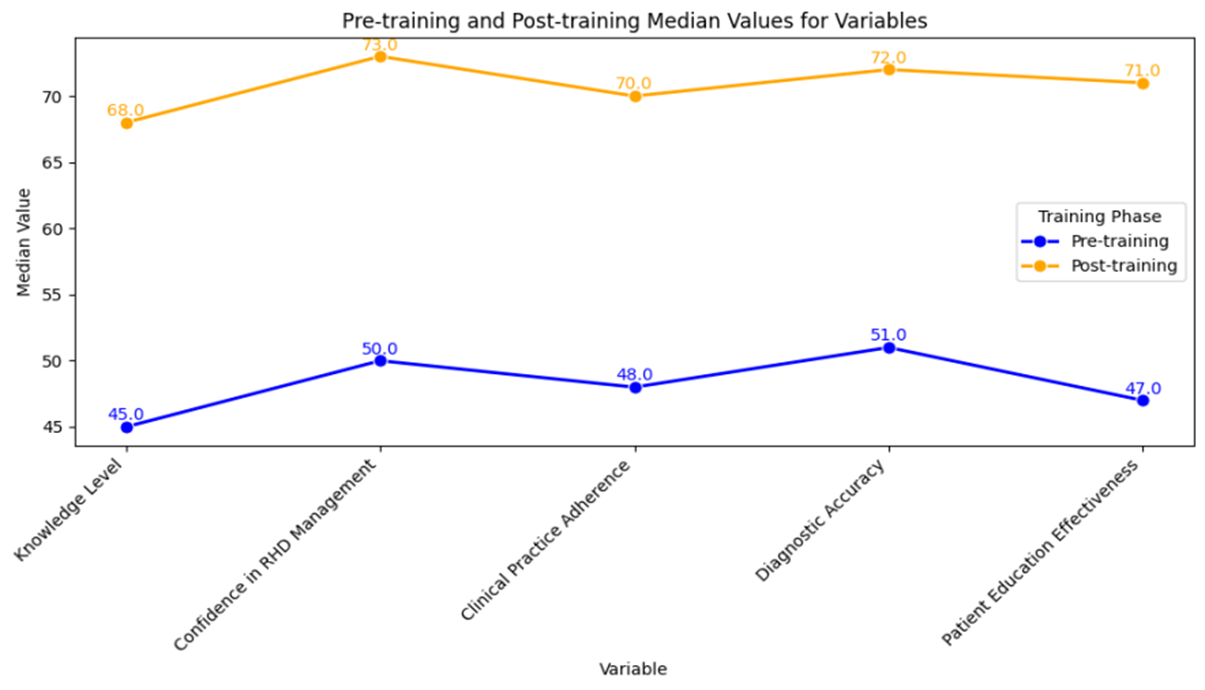
Figure 2. Pre- and Post-Comparison of Wilcoxon Signed-Rank Test Variables
ANCOVA is a statistical technique that combines the ideas of analysis of variance with regression. While statistically adjusting for the effects of one or more variables, it examines whether the means of a dependent variable change between groups. It removes the variability of the dependent variable that is observed about the covariates hence leaving the results of the independent variable. The covariate Pre-training Knowledge the dependent variable was affected as was found by an F-statistic of 10,5, p < 0,001 comparing initial knowledge level and post-training knowledge. The Training Effect also reached a statistical significance with an F-statistic of, 22,4, p<0,001. Therefore, confirmed that the training intervention influenced the dependent variable after accounting for prior knowledge. The partial η² expresses the percentage of variance accounted for by each factor. The covariate Pre-training Knowledge for 15 %, and the Training Effect explained the largest 30 % of the variance, evidencing the training’s influence on the differences observed during training. The significance of both the covariate and the training effect indicates that adjusting for baseline differences is critical for the assessment of interventions. Hence, through partially the effect of training, the analysis reduces variability and confirms that the intervention was responsible for enhancing the post-training knowledge and skills. Table 6 depicts the outcome of ANCOVA.
|
Table 6. Results of ANCOVA for Training Effectiveness |
||||||
|
Source |
Sum of Squares (SS) |
df |
Mean Square (MS) |
F-Statistic |
p-value |
Partial η² |
|
Pre-training Knowledge (Covariate) |
150,0 |
1 |
150,0 |
10,5 |
<0,001 |
0,15 |
|
Training Effect |
320,0 |
1 |
320,0 |
22,4 |
<0,001 |
0,30 |
|
Error |
1280,0 |
92 |
13,91 |
- |
- |
- |
|
Total |
1750,0 |
94 |
- |
- |
- |
- |
DISCUSSION
An effective outcome is highlighted in the statistical evaluation of the training program on enhancing the competencies of healthcare workers in the management of RHD. The paired t-test results present significant changes in all the studied variables, namely Knowledge Level, Clinical Practice Adherence, Diagnostic Accuracy, Confidence in RHD Management, and Patient Education Effectiveness with p-values less than 0,001. This indicates that the after-training scores were significantly higher than the initial training scores. These results are also supplemented by the Wilcoxon Signed-Rank Test, which shows a relatively high effect size from 0,60 to 0,64 which means that the impact of the intervention type was of medium to big effect. The Z-statistics of each variable demonstrate significant enhancements, with Patient Education Effectiveness as the major advancement. Thus, statistically significant differences between pre-training and post-test results show that the Pre-training Knowledge and the Training Effect had a significant F value and both the independent variables influenced the post-training outcomes, conditioning for the baseline difference. The value of The Training Effect was 0,30 which accounted for 30 % of the total variability, and the value of Pre-training Knowledge accounted for 15 % of the total variability, thus proving that the intervention made a significant difference. These findings imply that the training was useful in improving the knowledge and practice of healthcare workers dealing with RHD patients. The research findings reveal that consistently higher pre and post-test percentages in all the domains coupled with large-effect size, underline the importance of training endeavors in enhancing healthcare practices and patient outcomes in PHC.
CONCLUSIONS
The training program has produced a meaningful level of improvement in the management of RHD among the healthcare workforce in terms of their competence in terms of knowledge, clinical practices, diagnostic accuracy, and patient education. After using both pre-and post-training knowledge assessments together with clinic observations, significant improvements were noted in terms of meeting effective standards of RHD case identification and management by healthcare workers. Through the quantitative measures of the research with the use of ANCOVA, Paired t-tests, and Wilcoxon Signed-Rank Tests, it was estimated that all these enhancements are significant. This intervention holds the most promising impact on improving RHD outcomes in PHC and is more expansively beneficial to developing a stronger healthcare workers’ approach to handling RHD worldwide. A limitation of this study is its focus on primary healthcare settings, which could limit generalizability and subsequent research could include all healthcare settings and various settings with extended follow-up for evaluation of the course’s impact on RHD management results.
BIBLIOGRAPHIC REFERENCES
1. Enumah ZO, Boateng P, Bolman RM, Beyersdorf F, Zühlke L, Musoni M, Tivane A, ZillaP. Societies of futures past: examining the history and potential of international society collaborations in addressing the burden of rheumatic heart disease in the developing world. Frontiers in Cardiovascular Medicine. 2021 Nov 2;8:740745. https://doi.org/10.3389/fcvm.2021.740745
2. Lilyasari O, Prakoso R, Kurniawati Y, Roebiono PS, Rahajoe AU, Sakidjan I, Harimurti GM. Clinical profile and management of rheumatic heart disease in children and young adults at a tertiary cardiac center in Indonesia. Frontiers in Surgery. 2020 Aug 12;7:47. https://doi.org/10.3389/fsurg.2020.00047
3. Wyber R, Noonan K, Halkon C, Enkel S, Cannon J, Haynes E, Mitchell AG, Bessarab DC, Katzenellenbogen JM, Bond‐Smith D, Seth R. Ending rheumatic heart disease in Australia: the evidence for a new approach. Medical Journal of Australia. 2020 Nov;213:S3-1. https://doi.org/10.5694/mja2.50853
4. Jaiteh LE, Drammeh L, Anderson ST, Mendy J, Ceesay S, D’alessandro U, Carapetis J, Mirabel M, Erhart A. Rheumatic heart disease in The Gambia: clinical and valvular aspects at presentation and evolution under penicillin prophylaxis. BMC cardiovascular disorders. 2021 Dec;21:1-3. https://doi.org/10.1186/s12872-021-02308-8
5. Marijon E, Mocumbi A, Narayanan K, Jouven X, Celermajer DS. Persisting burden and challenges of rheumatic heart disease. European heart journal. 2021 Sep 7;42(34):3338-48.https://doi.org/10.1093/eurheartj/ehab407
6. Nyaaba GN, Masana L, Aikins AD, Beune E, Agyemang CJ. Factors hindering hypertension control: perspectives of front-line health professionals in rural Ghana. Public Health. 2020 Apr 1;181:16-23. https://doi.org/10.1016/j.puhe.2019.11.007
7. de Loizaga SR, Beaton AZ. Rheumatic fever and rheumatic heart disease in the United States. Pediatric annals. 2021 Mar 1;50(3):e98-104. https://doi.org/10.3928/19382359-20210221-01
8. Langlois EV, McKenzie A, Schneider H, Mecaskey JW. Measures to strengthen primary health-care systems in low-and middle-income countries. Bulletin of the World Health Organization. 2020 Nov 11;98(11):781. https://doi.org/10.2471/BLT.20.252742
9. Ndagire E, Kawakatsu Y, Nalubwama H, Atala J, Sarnacki R, Pulle J, Kyarimpa R, Mwima R, Kansiime R, Okello E, Lwabi P. Examining the Ugandan health system’s readiness to deliver rheumatic heart disease-related services. PLoS neglected tropical diseases. 2021 Feb 16;15(2):e0009164. https://doi.org/10.1371/journal.pntd.0009164
10. Rwebembera J, Beaton AZ, de Loizaga SR, Rocha RT, Doreen N, Ssinabulya I, Okello E, Fraga CL, Galdino BF, Nunes MC, Nascimento BR. The global impact of rheumatic heart disease. Current Cardiology Reports. 2021 Nov;23:1-0. https://doi.org/10.1007/s11886-021-01592-2
11. Belay W, Aliyu MH. Rheumatic heart disease is missing from the global health agenda. Annals of Global Health. 2021;87(1). https://doi.org/10.5334/aogh.3426
12. Vaughan G, Dawson A, Peek M, Carapetis J, Wade V, Sullivan E. Caring for Pregnant Women with Rheumatic Heart Disease: A Qualitative Study of Health Service Provider Perspectives. Global Heart. 2021;16(1). https://doi.org/10.5334/gh.1086
13. Haynes E, Walker R, Mitchell AG, Katzenellenbogen J, D’Antoine H, Bessarab D. Decolonizing Indigenous health: Generating a productive dialogue to eliminate rheumatic heart disease in Australia. Social Science & Medicine. 2021 May 1;277:113829. https://doi.org/10.1016/j.socscimed.2021.113829
14. Haynes E, Walker R, Mitchell AG, Katzenellenbogen J, D’Antoine H, Bessarab D. Decolonizing Indigenous health: Generating a productive dialogue to eliminate rheumatic heart disease in Australia. Social Science & Medicine. 2021 May 1;277:113829. https://doi.org/10.1186/s12913-020-05945-5
15. Voleti S, Okello E, Murali M, Sarnacki R, Majwala A, Ssembatya R, Bakka O, Namisanvu H, Njeri A, Matovu A, DeStigter K. The personal and clinical impact of screen-detected maternal rheumatic heart disease in Uganda: a prospective follow up study. BMC Pregnancy and Childbirth. 2020 Dec;20:1-0. https://doi.org/10.1186/s12884-020-03189-z
16. Kerrigan V, Kelly A, Lee AM, Mungatopi V, Mitchell AG, Wyber R, Ralph AP. A community-based program to reduce acute rheumatic fever and rheumatic heart disease in northern Australia. BMC health services research. 2021 Dec;21:1-5. https://doi.org/10.1186/s12913-021-07159-9
FINANCING
No financing.
CONFLICT OF INTEREST
None.
AUTHORSHIP CONTRIBUTION
Conceptualization: Ram Garg, Wakeel Ahmed, Deepak Kumar Parhi.
Data curation: Ram Garg, Wakeel Ahmed, Deepak Kumar Parhi.
Formal analysis: Ram Garg, Wakeel Ahmed, Deepak Kumar Parhi.
Drafting - original draft: Ram Garg, Wakeel Ahmed, Deepak Kumar Parhi.
Writing - proofreading and editing: Ram Garg, Wakeel Ahmed, Deepak Kumar Parhi.