doi: 10.56294/hl2022126
ORIGINAL
Research on health education strategies for improving student knowledge on infectious disease prevention
Investigación sobre estrategias de educación sanitaria para mejorar los conocimientos de los estudiantes sobre prevención de enfermedades infecciosas
Shailly
Gupta1 ![]() , Manashree Mane2
, Manashree Mane2 ![]() , Debashree Priyadarshini3
, Debashree Priyadarshini3
![]() , Ajab Singh Choudhary4
, Ajab Singh Choudhary4
![]()
1Arya College of Pharmacy. Jaipur, India.
2JAIN (Deemed-to-be University), Department of Forensic Science. Bangalore, India.
3IMS and SUM Hospital, Siksha ‘O’ Anusandhan (Deemed to be University), Department of Paediatrics. Bhubaneswar, India.
4Noida International University, School of Allied Health Sciences. Greater Noida, India.
Cite as: Gupta S, Mane M, Priyadarshini D, Singh Choudhary A. Research on Health Education Strategies for Improving Student Knowledge on Infectious Disease Prevention. Health Leadership and Quality of Life. 2022; 1:126. https://doi.org/10.56294/hl2022126
Submitted: 11-08-2022 Revised: 29-10-2022 Accepted: 14-12-2022 Published: 15-12-2022
Editor:
PhD.
Prof. Neela Satheesh ![]()
ABSTRACT
The increasing number of infectious diseases in public settings emphasizes the necessity of efficient health education programs to give students fundamental knowledge and preventative skills. This investigates successful health education strategies to improve students’ learning and behavior about preventing infectious diseases. Data, including socioeconomic characteristics, were gathered from 1250 students. Before implementing health education techniques, baseline information is gathered from participants through a survey to assess their initial level of infectious disease prevention knowledge and behaviors. The same tests are conducted again following the intervention to evaluate if students have any improvements based on the health education strategy. The investigation assesses several educational approaches, including digital learning tools, classroom lectures, and peer-led activities, to establish their importance in increasing awareness of hygiene habits, disease transmission, and prevention measures. Using SPSS, statistical techniques like regression analysis and paired t-tests are utilized to compare pre- and post-intervention in health education. The findings indicate that interactive and technology-based techniques significantly improve knowledge retention and encourage the adoption of preventive actions. Furthermore, peer-led education had a favourable impact on participation and behavior modification. This investigation emphasizes the value of targeted, engaging, and evidence-based health education programs in enhancing student knowledge and behavior about infectious disease prevention. It suggests incorporating such measures into school curricula to strengthen resilience to disease outbreaks and enhance public health outcomes.
Keywords: Infectious Diseases; Knowledge; Health Education Strategies; Behavior; Prevention.
RESUMEN
El creciente número de enfermedades infecciosas en los entornos públicos pone de relieve la necesidad de programas eficaces de educación sanitaria para proporcionar a los estudiantes conocimientos fundamentales y habilidades preventivas. En este trabajo se investigan estrategias eficaces de educación sanitaria para mejorar el aprendizaje y el comportamiento de los estudiantes en materia de prevención de enfermedades infecciosas. Se recopilaron datos, incluidas las características socioeconómicas, de 1250 estudiantes. Antes de poner en práctica las técnicas de educación sanitaria, se recoge información de referencia de los participantes mediante una encuesta para evaluar su nivel inicial de conocimientos y conductas de prevención de enfermedades infecciosas. Las mismas pruebas se vuelven a realizar tras la intervención para evaluar si los alumnos presentan alguna mejora gracias a la estrategia de educación sanitaria. La investigación evalúa varios enfoques educativos, incluidas herramientas de aprendizaje digital, conferencias en el aula y actividades dirigidas por compañeros, para establecer su importancia a la hora de aumentar la concienciación sobre los hábitos de higiene, la transmisión de enfermedades y las medidas de prevención. Utilizando SPSS, se emplean técnicas estadísticas como el análisis de regresión y las pruebas t pareadas para comparar la educación sanitaria antes y después de la intervención. Las conclusiones indican que las técnicas interactivas y basadas en la tecnología mejoran significativamente la retención de conocimientos y fomentan la adopción de medidas preventivas. Además, la educación dirigida por iguales tuvo un impacto favorable sobre la participación y la modificación del comportamiento. Esta investigación subraya el valor de los programas de educación sanitaria específicos, atractivos y basados en pruebas para mejorar los conocimientos y el comportamiento de los alumnos en materia de prevención de enfermedades infecciosas. Sugiere incorporar tales medidas a los planes de estudios escolares para reforzar la capacidad de resistencia a los brotes de enfermedades y mejorar los resultados en materia de salud pública.
Palabras clave: Enfermedades infecciosas; Conocimiento; Estrategias de educación sanitaria; Comportamiento; Prevención.
INTRODUCTION
Enlightening student’s knowledge on communicable disease Inhibition has a crucial role in today’s world, where public health faces frequent challenges from new diseases and ongoing risks from established infections.(1) As the world becomes more connected, the spread of infectious diseases has turned into a key issue affecting people, communities, and nations.(2) It also helps support wider efforts to manage public health. Students, particularly those at younger ages, represent a critical population in combatting infectious diseases, due to the future workforce; it can strongly impact families and communities in their society.(3) For instance, understanding key concepts, such as the significance and methods of cleanliness, the value and modes of vaccination, and healthy practices- could have a broad impact over time-hazardous periods as young people begin forming lifestyles and thinking habits.(4)
The educational environment provides the perfect setting to acquire these skills because students transform into learning objects after the individual enter this structured learning environment that modern educational approaches, including habit development strategies, have introduced for younger students.(5) Therefore, introducing respectable lessons enables such little learners to grow in information and healthier judgments about their health, with some optimism spread down to communities, in terms of not letting diseases spread.(6) Additionally, increased awareness of infectious diseases and their prevention gives students a sense of responsibility and social consciousness.(7) When young individuals are well informed, they become health advocates, sharing their knowledge with peers, families, and even communities. In the long run, fostering a culture of prevention will not only protect individuals but also strengthen the resilience of communities to public health risks.(8) This investigation aims to evaluate and improve students’ knowledge and practices regarding infectious disease prevention by examining different health education strategies, and their impact on awareness and preventive behaviors.
The training program that would enhance Korean nursing students’ understanding and their confidence in managing assignments and learning experiences was investigated in a study.(9) The experimental group produced better results than the control group in the areas of learner satisfaction (t=-5,59 p<0,001) and high-risk neonatal contamination control self-efficacy (t=-2,16 p=0,018). By using an inductive thematic saturation method, the investigators found data after analysing the reports from 33 undergraduate nursing students.(10) The findings indicated that there was some disagreement among students regarding the efficacy of information systems and state agencies. Every student discussed disseminating false information on social media and made an effort to use only pertinent data.
Both anxiety and uncertainty levels about the coronavirus in 2019, alongside how students had worried over that period, that were examined in a study.(11) The results show that knowledge about the virus reduced anxiety and panic, increased unwanted suspicion, and intolerance. It showed that age, gender, and the type of college the students attended could explain the fear levels. Human Immunodeficiency Virus (HIV) became more common across the years from 2001 to 2018 and risk increased for older men who intimate with Men (MSM) compared to younger MSM that had been discussed in a study.(12) The experimental result showed that effective healthcare policy must address the HIV needs of high-risk groups through proven treatment and monitoring methods.
Personal Protective Equipment (PPE) equipment had shielded Health Care Workers (HCW) from disease contact and protected them from getting contamination, as evaluated in a study.(13) The efficiency of PPE removal depends directly on the design aspects of protective equipment through correct sizing and the selection of fasteners. The investigation assessed(14) south Indian undergraduate medical, dental, and nursing students on their understanding and acceptance of the Human Papillomavirus (HPV) vaccination. The result showed significant knowledge gaps in many areas, suggesting that medical schools needed to include more teaching about HPV and the benefits of vaccination.
The effect of educating patients about type 2 diabetes tests measuring their knowledge gain, changes in beliefs, and blood sugar control practices was evaluated in a study.(15) From the results of the investigation, the end cases experienced a range of 10,28 ± 1,78 increases in their knowledge and actions, which proved different than their initial results.
METHOD
The investigation has evaluated healthcare education methods to teach students better ways to defend against infectious diseases. Statistical methods and investigations processed data are collected from 1250 students. The educational approaches have consisted of digital tools combined with classroom teaching and peer workshops. Students learned more due to digital and interactive approaches and participated more in peer-led learning. It demonstrated that students need interactive health education programs in their schools.
Data Collection
The investigation with 1250 students requires gathering data through pre intervention which will evaluate participants’ understanding and actual practices related to disease prevention. To explore three main topics related to hygiene behaviours, disease transmission understanding, and current protective methods. The initial assessment through research needs demographic participant information that includes age details and gender alongside socio-economic data for factor discrimination. The same set of questions will be asked during a post investigation after the intervention to check for improvements in participant knowledge and actions. Table 1 describes the demographic data of variables. The distribution of participants by health knowledge before intervention and participation in health programs are represented as (a) and (b) in figure 1.
|
Table 1. The Demographic Data of variables |
|||
|
Demographic Variable |
Categories |
Frequency (n) |
Percentage (%) |
|
Gender |
Male |
620 |
49,6 |
|
|
Female |
630 |
50,4 |
|
Age Group |
10-12 Years |
300 |
24,0 |
|
|
13-15 Years |
550 |
44,0 |
|
|
16-18 Years |
400 |
32,0 |
|
Previous Health Education |
Yes |
450 |
36 |
|
|
No |
800 |
64 |
|
Previous illness |
Yes |
600 |
48 |
|
|
No |
650 |
52 |
|
Awareness Hygiene |
Good |
450 |
36 |
|
|
Average |
550 |
44 |
|
|
Poor |
250 |
20 |
|
Health Knowledge Before Intervention |
Basic |
500 |
40 |
|
|
Intermediate |
600 |
48 |
|
|
Advanced |
150 |
12 |
|
Participation in Health Programs |
Yes |
450 |
36 |
|
|
No |
800 |
64 |
|
Technology Access |
Yes |
850 |
68 |
|
|
No |
400 |
32 |
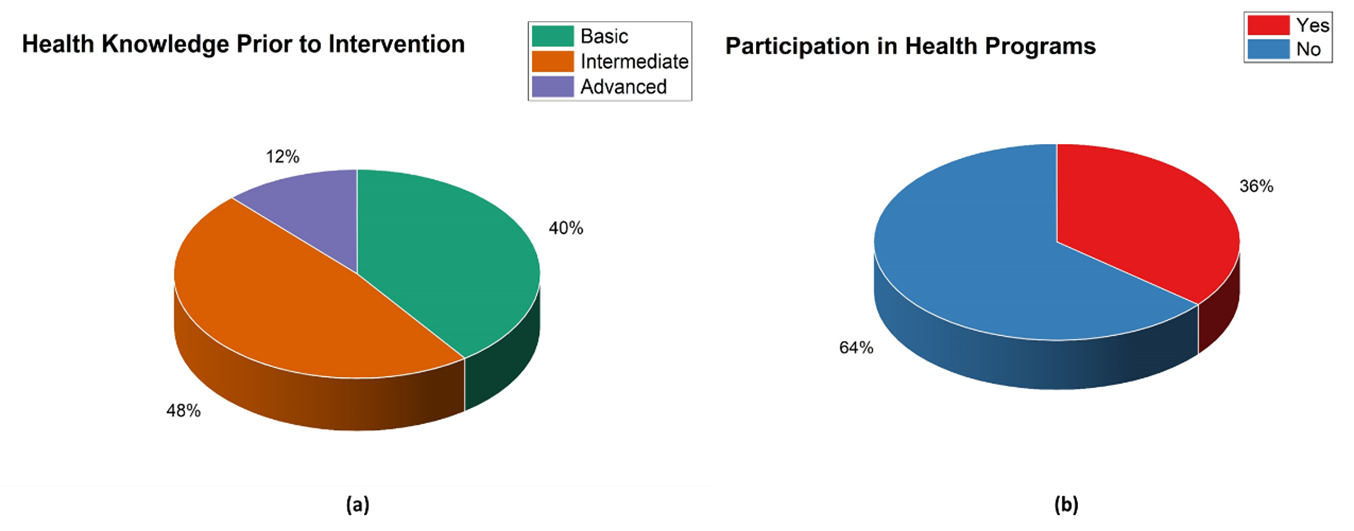
Figure 1. Distribution of Participants by Demographic Variables (a) Health Knowledge before Intervention and (b) Participation in Health Programs
Intervention
The intervention incorporates three primary health education techniques. Education through technology uses apps together with videos and interactive modules to offer students visual learning experiences that both enhance accessibility and engage students more effectively. Health professionals conduct awesome classroom lectures to teach prevention knowledge in formal learning spaces. As part of the intervention approach peer-led activities allow students to guide discussions while conducting role-plays that enhance both their behavior change efforts and their ability to retain concepts. A combination of these strategies works to enhance both student comprehension of infectious disease prevention and their actual prevention practices.
Structure of Questionnaires
Knowledge of Infectious Disease Prevention: five questions are included in this part to measure the students’ understanding of disease prevention methods, transmission routes, and effective hygiene practices to reduce infection risks.
Preventive Behaviour Adoption: this section contains four questions that assess the students’ consistent engagement in actions like hand washing, mask-wearing, and avoiding close contact to prevent diseases.
Hygiene Habits: it contains five questions that are used to evaluate students’ daily routines in maintaining cleanliness, such as hand washing, disinfecting surfaces, and personal space hygiene.
Peer Influence: four questions are included in this section to examine the role of peer-led activities and interactions in influencing students’ knowledge and behavior toward disease prevention.
Technology Engagement: in this section, four questions are used to track the purpose of digital tools and resources by students Along with them to enhance understanding and retention of disease prevention knowledge. The sample questionnaires are shown in table 2.
|
Table 2. Sample Questionnaires |
||
|
Variable |
Number of Questions |
Survey Questions |
|
Knowledge of Infectious Disease Prevention |
5 |
How familiar are you with common methods of preventing infectious diseases? Can you list three diseases that can be transmitted through close contact? What are the primary ways to reduce the spread of respiratory diseases? Do you know how long viruses like the flu can survive on surfaces? How often should you wash your hands to reduce the risk of infection? |
|
Preventive Behaviour Adoption |
4 |
How often do you wash your hands during the day? Do you wear a mask when feeling unwell or during flu season? How often do you avoid close contact with people who are sick? Do you use hand sanitizer when soap and water are unavailable? |
|
Hygiene Habits |
5 |
How regularly do you wash your hands with soap and water? Do you clean and disinfect your items (e.g., phone, keyboard) regularly? How often do you clean your living and study spaces? Do you cover your mouth and nose when coughing or sneezing? How often do you use sanitizers or wipes on shared surfaces? |
|
Peer Influence |
4 |
How much influence do your friends have on your decision to adopt hygiene practices? Are you more likely to wash your hands if your peers are doing it? Do you participate in peer-led activities about health or disease prevention? How often do you discuss health practices and prevention with your peers? |
|
Technology Engagement |
4 |
How often do you use digital learning tools (apps, websites) to learn about hygiene and disease prevention? Do you find online educational resources helpful in understanding disease prevention? How often do you complete interactive modules or quizzes related to health and hygiene practices? Do you believe using technology-based learning tools helps you remember hygiene and disease prevention tips? |
Statistical Assessment
The research uses IBM SPSS Statistics 25 to test how health education approaches enhance knowledge and behavior to prevent infectious diseases. The effect of health education strategies with variables on student knowledge development and behavioral transformations becomes measurable through regression analysis. A p-value below 0,05 helped to detect if students gained new health knowledge and started healthier life practices through the health education program. Paired t-test evaluation measures how well participants learned from the program and how their actions evolved. ANOVA analysis will show if the differences in group results stand up to statistical review.
RESULTS
The exploration aimed to assess the impact on key variables, such as knowledge of prevention methods, preventive behaviors, hygiene habits, peer influence, and technology engagement. Statistical analyses, which include Regression analysis, paired t-tests, and Analysis of Variance (ANOVA) are used to assess the statistical connotation of outcomes of the intervention.
Regression Analysis
Data analysis demonstrated how students gained important disease protection skills after participating in the program. The participants showed significant improvement in their ability to recognize the knowledge of infectious disease prevention from 0,45 pre-intervention to 0,70 post-intervention through a β coefficient of 0,55 (P=0,001). Students increased their preventive behavior adoption marker from 0,50 to 0,75 when measured at both endpoints (β = 0,60, p = 0,002) and improved their Hygiene habits from 0,40 to 0,68 (β = 0,50, p = 0,003). The results demonstrate significant improvement in Peer Influence measurements from an initial 0,35 to 0,65 (p = 0,004). Technology engagement quality in the program showed the strongest improvement increasing from 0,60 to 0,80 with a link of 0,65 (p = 0,001). It shows that students learned more about preventing diseases and matched their new knowledge with proper behavior. Figure 2 and table 3 illustrate the Pre and Post Intervention variables using regression analysis.
|
Table 3. Regression Analysis Test for variables in Pre and Post Intervention |
||||
|
Variable |
Pre-Intervention Score (R2) |
Post-Intervention Score (R2) |
β (beta) Coefficient |
p-value |
|
Knowledge of Infectious Disease Prevention |
0,45 |
0,70 |
0,55 |
0,001 |
|
Preventive Behaviour Adoption |
0,50 |
0,75 |
0,60 |
0,002 |
|
Hygiene Habits |
0,40 |
0,68 |
0,50 |
0,003 |
|
Peer Influence |
0,35 |
0,65 |
0,52 |
0,004 |
|
Technology Engagement |
0,60 |
0,80 |
0,65 |
0,001 |
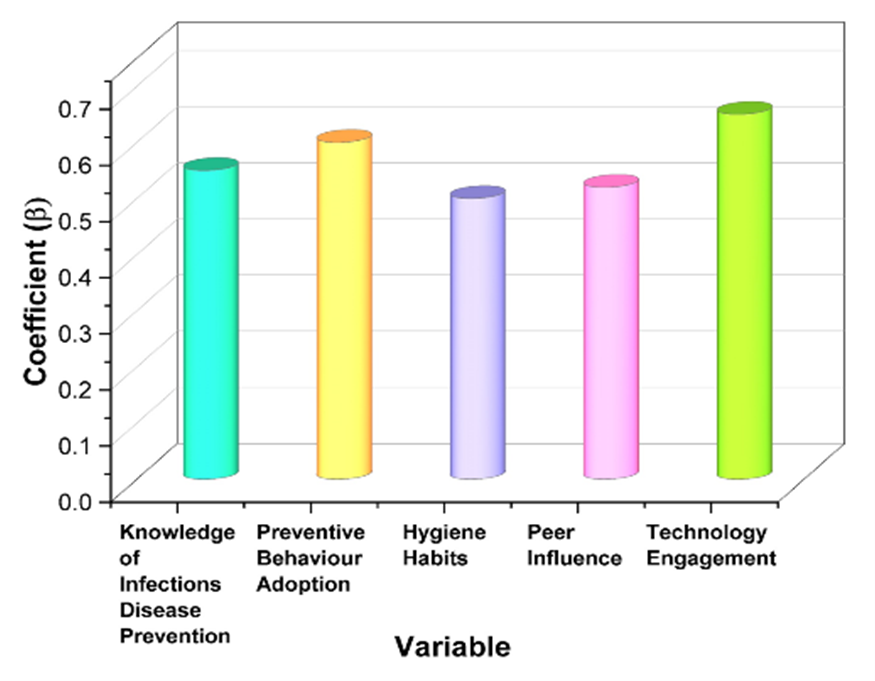
Figure 2. Graphical Representation of variables in Regression Analysis
Paired t-tests
The paired t-test data shows that students demonstrated better knowledge and improved behavior in stopping infectious diseases after taking part in the program. Following the intervention, students achieved a significant knowledge boost in preventing infectious diseases from 4,2 pre-test to 6,9 post-test with strong statistical support. A positive shift in preventive behavior adoption emerged between measurements from 3,5 points to 6,4 points (t-value = 13,8, p = 0,002). In the investigation, participants demonstrated better hygiene practices from 3,4 to 6,1 when measured through statistical testing (t-value = 12,5, p = 0,001). The participants showed strong engagement with peers since their responses on peer influence moved from 3,2 before training to 5,8 after training (t-value = 14,0, p = 0,001). Technology engagement scores increased from 4,5 to 7,2 and this difference was highly significant with a t-value of 16,0 at p<0,001. The result shows that the intervention produced improved knowledge and behavior outcomes because all test results had p-values smaller than 0,05. The paired t-tests of the variables for pre- and post-intervention are shown in figure (3) and table (4).
|
Table 4. Paired t-test for variables in Pre and Post Evaluation |
||||
|
Variable |
Pre-Intervention Mean |
Post-Intervention Mean |
t-value |
p-value |
|
Knowledge of Infectious Disease Prevention |
4,2 |
6,9 |
15,2 |
0,001 |
|
Preventive Behaviour Adoption |
3,5 |
6,4 |
13,8 |
0,002 |
|
Hygiene Habits |
3,4 |
6,1 |
12,5 |
0,001 |
|
Peer Influence |
3,2 |
5,8 |
14,0 |
0,001 |
|
Technology Engagement |
4,5 |
7,2 |
16,0 |
0,001 |
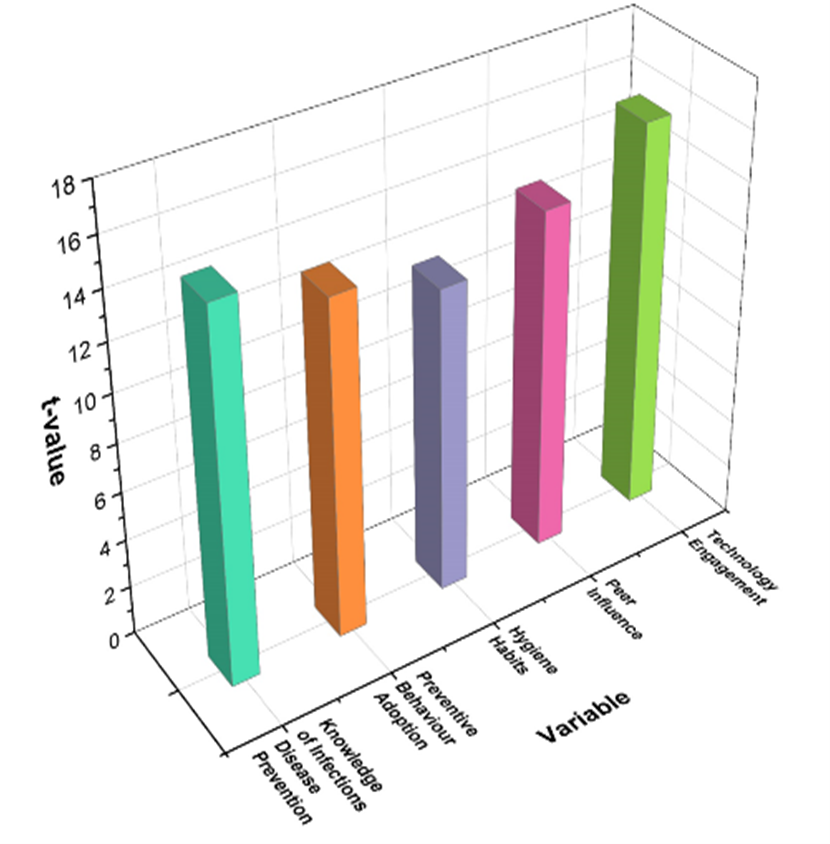
Figure 3. Graphical Representation of variables in Paired t-test Analysis
ANOVA Test
ANOVA shows major positive changes in the investigation results after the treatment. Students gained an extensive understanding of how to prevent infectious diseases from 4,2 to 6,9 based on test results with an F-value of 45,32 and strong statistical relevance (significance level 0,001). The findings show that the percentage of students’ preventive behavior adoption is from 3,5 to 6,4 (p = 0,001). Students showed stronger hygiene habits in all classes with a rise from 3,4 to 6,1 while maintaining their statistical significance (F = 47,10 and p = 0,001). Student responses to Peer Influence grew substantially from 3,2 to 5,8 through the experimental approach (F-value = 50,00 and p < 0,001). Students interacted more with technological resources following the program adjustment as technology engagement almost doubled (F-value = 48,56, p = 0,001). The findings show that the approach strongly changed students’ disease prevention behaviors and information at p-values under 0,05. Figure (4) and table (5) visualize the ANOVA test of the variables for pre- and post-intervention.
|
Table 5. ANOVA test for variables in Pre and Post Evaluation |
||||
|
Variable |
Pre-Intervention Mean |
Post-Intervention Mean |
f-value |
p-value |
|
Knowledge of Infectious Disease Prevention |
4,2 |
6,9 |
45,32 |
0,001 |
|
Preventive Behaviour Adoption |
3,5 |
6,4 |
42,18 |
0,001 |
|
Hygiene Habits |
3,4 |
6,1 |
47,10 |
0,001 |
|
Peer Influence |
3,2 |
5,8 |
50,00 |
0,001 |
|
Technology Engagement |
4,5 |
7,2 |
48,56 |
0,001 |
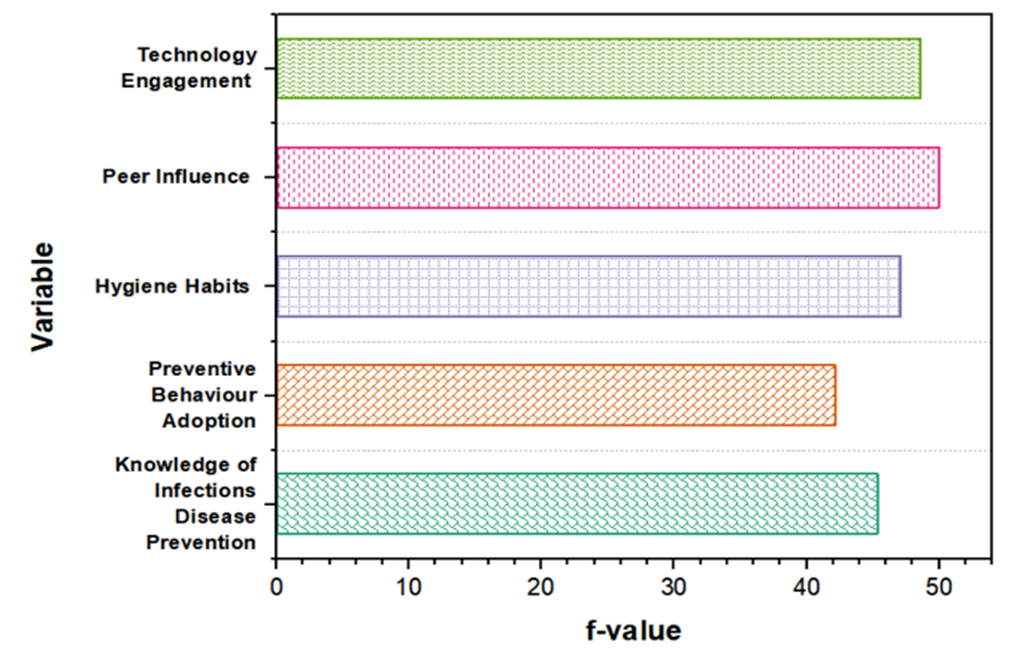
Figure 4. Visual Representation of variables in the ANOVA test
Discussion
The statistical analysis demonstrated that the health education program optimally benefits students regarding infection prevention knowledge and habits. In the regression analysis, all intervention post-scores are significantly and considerably higher: The post-intervention variables showing the highest impact include technology engagement with an R² value of 0,80 and β value of 0,65 followed by preventive behavior adoption with R² at 0,75 and β rate of 0,60 and Knowledge of infectious disease prevention with R² = 0,70 and β = 0,55. Research data in the Paired t-test revealed that technology engagement (Mean = 7,2, t = 16,0) achieved the most significant improvement alongside Knowledge of infectious disease prevention (Mean = 6,9, t = 15,2) and peer influence (Mean = 5,8, t = 14,0) which demonstrated statistical significance in this case. This large and significant increase implies that students actively engaged with digital learning tools and contributed to their better understanding of disease prevention. The ANOVA results indicate peer influence (F = 50,00, p = 0,001) and technology engagement (F = 48,56, p = 0,001) together with hygiene habits (F = 47,10, p = 0,001) achieved the most significant improvements. These variables show statistically meaningful changes in student behavior together with knowledge retention. Generally, all variables experienced high improvements following the intervention with technology engagement proving to have the highest impacts. The findings were significant on all tests to establish that an all-rounded strategy that incorporates the use of digital tools, influence by peers, and class activities best boosts students’ understanding and practices toward preventing infectious diseases. These findings establish the relevance of such strategy in improving education curricula and public health.
CONCLUSIONS
The analysis has highlighted the essentiality of health education interventions by showing considerably good improvement in terms of students’ knowledge and their behaviors regarding preventing infectious diseases. Regression analysis revealed that the post-intervention R² was a maximum of 0,80 and the β coefficient for Technology Engagement was 0,65 (p = 0,001), which emphasizes the superior efficiency of digital learning tools. The largest mean improvement the paired t-test showed and resulted in technology engagement, which expanded from 4,5 to 7,2 (t-value = 16,0, p = 0,001). According to the analysis, ANOVA also confirmed improved changes across variables, especially about technology engagement at F-value = 48,56, and p = 0,001. These findings suggest that incorporating interactive digital tools, along with peer-led activities and classroom lectures, can effectively enhance students’ knowledge and behavior related to infectious disease prevention. For future analysis, further studies could explore long-term retention of knowledge and behavior change, assess the impact of different digital tools, and evaluate the intervention’s effectiveness across various demographic groups.
BIBLIOGRAPHIC REFERENCES
1. Sun Y, Wang D, Han Z, Gao J, Zhu S, Zhang H. Disease prevention knowledge, anxiety, and professional identity during COVID-19 pandemic in nursing students in Zhengzhou, China. Journal of Korean Academy of Nursing. 2020 50(4):533-40. https://doi.org/10.4040/jkan.20125
2. Johnson MA, Jones BM, Heil EL, Stover KR, Trone S, Fulford M, Bland CM. Self-perceived knowledge and confidence regarding infectious diseases of advanced pharmacy practice experience students. Currents in Pharmacy Teaching and Learning. 2019 Nov 1; 11(11):1095-102. https://doi.org/10.1016/j.cptl.2019.07.019
3. Adou AA, Napolitano F, Vastola A, Angelillo IF. Travelers’ knowledge, attitudes, and behavior related to infectious diseases in Italy. PloS one. 2019 Apr 12; 14(4):e0215252. https://doi.org/10.1371/journal.pone.0215252
4. Goni MD, Naing NN, Hasan H, Wan-Arfah N, Deris ZZ, Arifin WN, Hussin TM, Abdulrahman AS, Baaba AA, Arshad MR. Development and validation of knowledge, attitude and practice questionnaire for prevention of respiratory tract infections among Malaysian Hajj pilgrims. BMC public health. 2020 Dec; 20:1-0. https://doi.org/10.1186/s12889-020-8269-9
5. Alao MA, Durodola AO, Ibrahim OR, Asinobi OA. Assessment of Health Workers’ Knowledge, Beliefs, Attitudes, and Use of Personal Protective Equipment for Prevention of COVID‐19 Infection in Low‐Resource Settings. Advances in Public Health. 2020 2020(1):4619214. https://doi.org/10.1155/2020/4619214
6. Abdel Wahed WY, Hefzy EM, Ahmed MI, Hamed NS. Assessment of knowledge, attitudes, and perception of health care workers regarding COVID-19, a cross-sectional study from Egypt. Journal of community health. 2020 Dec; 45(6):1242-51. https://doi.org/10.1007/s10900-020-00882-0
7. Azevedo MM, Ricardo E, Teixeira Dos Santos R, Pina-Vaz C, Rodrigues AG. “Filling a gap: knowledge in health related science for middle school students in formal and informal contexts. Journal of Biological Education. 2020 Mar 14; 54(2):129-46. https://doi.org/10.1080/00219266.2018.1546764
8. Ataş O, Yildirim TT. Evaluation of knowledge, attitudes, and clinical education of dental students about COVID-19 pandemic. PeerJ. 2020 Jul 29; 8:e9575. https://doi.org/10.7717/peerj.9575
9. Yu M, Yang M, Ku B, Mann JS. Effects of virtual reality simulation program regarding high-risk neonatal infection control on nursing students. Asian Nursing Research. 2021 Aug 1; 15(3):189-96. https://doi.org/10.1016/j.anr.2021.03.002
10. Lovrić R, Farčić N, Mikšić Š, Včev A. Studying during the COVID-19 pandemic: A qualitative inductive content analysis of nursing students’ perceptions and experiences. Education sciences. 2020 Jul 21; 10(7):188. https://doi.org/10.3390/educsci10070188
11. Elsharkawy NB, Abdelaziz EM. Levels of fear and uncertainty regarding the spread of coronavirus disease (COVID‐19) among university students. Perspectives in Psychiatric Care. 2021 Jul; 57(3):1356-64. https://doi.org/10.1111/ppc.12698
12. Dong MJ, Peng B, Liu ZF, Ye QN, Liu H, Lu XL, Zhang B, Chen JJ. The prevalence of HIV among MSM in China: a large-scale systematic analysis. BMC infectious diseases. 2019 Dec; 19:1-20. https://doi.org/10.1186/s12879-019-4559-1
13. Baloh J, Reisinger HS, Dukes K, da Silva JP, Salehi HP, Ward M, Chasco EE, Pennathur PR, Herwaldt L. Healthcare workers’ strategies for doffing personal protective equipment. Clinical Infectious Diseases. 2019 Sep 13; 69(Supplement_3):S192-8. https://doi.org/10.1093/cid/ciz613
14. Shetty S, Prabhu S, Shetty V, Shetty AK. Knowledge, attitudes and factors associated with acceptability of human papillomavirus vaccination among undergraduate medical, dental and nursing students in South India. Human vaccines & immunotherapeutics. 2019 Aug 3;15(7-8):1656-65. https://doi.org/10.1080/21645515.2019.1565260
15. Chawla SP, Kaur S, Bharti A, Garg R, Kaur M, Soin D, Ghosh A, Pal R. Impact of health education on knowledge, attitude, practices and glycemic control in type 2 diabetes mellitus. Journal of family medicine and primary care. 2019 Jan 1;8(1):261-8. https://doi.org/10.4103/jfmpc.jfmpc_228_18
FINANCING
No financing.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORSHIP CONTRIBUTION
Data curation: Shailly Gupta, Manashree Mane, Debashree Priyadarshini, Ajab Singh Choudhary.
Methodology: Shailly Gupta, Manashree Mane, Debashree Priyadarshini, Ajab Singh Choudhary.
Software: Shailly Gupta, Manashree Mane, Debashree Priyadarshini, Ajab Singh Choudhary.
Drafting - original draft: Shailly Gupta, Manashree Mane, Debashree Priyadarshini, Ajab Singh Choudhary.
Writing - proofreading and editing: Shailly Gupta, Manashree Mane, Debashree Priyadarshini, Ajab Singh Choudhary.