doi: 10.56294/hl2022112
ORIGINAL
Assessing the Effectiveness of Health Promotion in Enhancing Quality of Life in Heart Failure Patients
Evaluación de la eficacia de la promoción de la salud para mejorar la calidad de vida de los pacientes con insuficiencia cardíaca
Renuka Jyothi. S1 ![]() , Suresh Kumar Behera2
, Suresh Kumar Behera2 ![]() , Indu Singh3
, Indu Singh3 ![]() , Shankar Lal Soni4
, Shankar Lal Soni4 ![]()
1JAIN (Deemed-to-be University), Department of Biotechnology and Genetics. Bangalore, India.
2IMS and SUM Hospital, Siksha ‘O’ Anusandhan (Deemed to be University), Department of Cardiology. Bhubaneswar, India.
3Noida International University, School of Education. Greater Noida, India.
4Arya College of Pharmacy, Jaipur, India.
Cite as: Renuka JS, Behera SK, Singh I, Soni SL. Assessing the Effectiveness of Health Promotion in Enhancing Quality of Life in Heart Failure Patients. Health Leadership and Quality of Life. 2022; 1:112. https://doi.org/10.56294/hl2022112
Submitted: 08-08-2022 Revised: 26-10-2022 Accepted: 12-12-2022 Published: 13-12-2022
Editor:
PhD.
Prof. Neela Satheesh ![]()
ABSTRACT
Heart failure (HF) is a chronic and debilitating condition that adversely affects patients’ quality of life (QoL). While health promotion interventions, particularly self-management strategies, are widely acknowledged as potential tools for improving QoL in HF patients, existing studies have yielded mixed results, with limited evidence on long-term effectiveness. Prior research on health promotion interventions for HF patients often suffers from small sample sizes, short follow-up periods, and inconsistent measures of QoL. Furthermore, many studies have not fully integrated multidimensional approaches, considering both physical and psychosocial aspects of health. A randomized controlled trial (RCT) was conducted with sixty HF patients and randomly allocated to either an intervention group (int grp) or a control group (Ctrl grp) through stratified block sampling. The int grp received a six-stage self-management promotion model, encompassing education on medication adherence, physical activity, dietary modifications, and psychosocial support. QoL was assessed using the structuredquestionnaire for HF patients at three-time points: baseline, immediate post-intervention, and one-month post-intervention. Statistical analysis involving ANOVA revealed significant improvement in the socioeconomic subscale scores of the HF questionnaire within the int grp. However, no significant differences were observed between the int grp and ctrl grp across the other subscales or the overall QoL score at any of the three-time points (p < 0,05). The self-management promotion model results in significant improvements in the overall QoL of HF patients.
Keywords: Heart Failure (HF); Structured Questionnaire; Quality of Life (QoL); Self-Management Promotion Model.
RESUMEN
La insuficiencia cardíaca (IC) es una enfermedad crónica y debilitante que afecta negativamente a la calidad de vida de los pacientes. Aunque las intervenciones de promoción de la salud, en particular las estrategias de autocuidado, están ampliamente reconocidas como herramientas potenciales para mejorar la CdV de los pacientes con IC, los estudios existentes han arrojado resultados dispares, con pruebas limitadas sobre la eficacia a largo plazo. Las investigaciones previas sobre intervenciones de promoción de la salud para pacientes con IC a menudo adolecen de tamaños de muestra pequeños, periodos de seguimiento cortos y mediciones inconsistentes de la CdV. Además, muchos estudios no han integrado plenamente enfoques multidimensionales, teniendo en cuenta tanto los aspectos físicos como psicosociales de la salud. Se realizó un ensayo controlado aleatorizado (ECA) con sesenta pacientes con IC y se les asignó aleatoriamente a un grupo de intervención (grp int) o a un grupo de control (grp Ctrl) mediante un muestreo estratificado por bloques. El grupo int recibió un modelo de promoción de la autogestión de seis etapas, que abarcaba la educación sobre el cumplimiento de la medicación, la actividad física, las modificaciones dietéticas y el apoyo psicosocial. La calidad de vida se evaluó mediante el cuestionario estructurado para pacientes con IC en tres momentos: al inicio, inmediatamente después y un mes después de la intervención. El análisis estadístico mediante ANOVA reveló una mejora significativa en las puntuaciones de la subescala socioeconómica del cuestionario de IC dentro del grupo int. Sin embargo, no se observaron diferencias significativas entre el grupo int y el grupo ctrl en las demás subescalas ni en la puntuación global de la CdV en ninguno de los tres momentos (p < 0,05). El modelo de promoción del autocontrol produce mejoras significativas en la CdV global de los pacientes con IC.
Palabras clave: Insuficiencia Cardiaca (IC); Cuestionario Estructurado; Calidad de Vida (CdV); Modelo de Promoción de la Autogestión.
INTRODUCTION
A leading cause of death and morbidity, heart failure (HF) is a growing public health issue. When the heart cannot pump enough blood to the body, it is called HF. This is typically brought on by high blood pressure, diabetes, or other heart diseases.(1) Many HF patients experience reduced functional ability, a low quality of life (QoL), and early death despite evidence-based treatments.(2) The fight against HF is placing an unprecedented financial strain on the healthcare system, and symptoms can range from asymptomatic to significantly impairing functioning.Estimation of prognosis in HF is essential because patients who are at a higher threat of adverse effects can gain from more frequent monitoring and aggressive treatment.(3) Though advances in medical treatment have improved survival rates, most HF patients continue to enjoy a poor QoL because of the long-term effects of their condition. This has highlighted the need for holistic approaches that go beyond clinical interventions to address the broader aspects of living with HF.(4)
Therefore, health promotion has been a critical consequence in improving patients' outcomes and has focused more on empowering such patients to cope with their situation and lead healthy, productive, and fulfilling lives. Unlike conventional medical care, the approach of health promotion focuses on proactive lifestyle change, self-care practices, and psychosocial support rather than symptom management alone. These interventions are to allow patients to actively manage their conditions, thereby ultimately improving their QoL while reducing the burden on the healthcare systems.(5) Educational programs, behavioral interventions, and psychosocial support are critical health promotion approaches for HF. The educational intervention empowers the patient with important knowledge about the condition, which includes medication compliance, dietary guidance, and maintaining regular exercise. Behavioral interventions promote healthier behaviors, including increased smoking cessation, stress management, and physical activity. Psychosocial support, through counseling or peer support groups, addresses the emotional challenges of living with HF, such as anxiety, depression, and social isolation.(6)
Technology-based approaches, such as telehealth and apps, also allow further growth in terms of reach and accessibility for health promotion programs, making them more inclusive and adaptive to the needs of individuals.(7) As health promotion strategies in HF care continue to move forward, several challenges have been identified. Socioeconomic factors, healthcare disparities, and variations in patient adherence limit the effectiveness of these interventions. In addition, the heterogeneity of HF patients in terms of age, disease severity, and comorbidities requires individual approaches to ensure successful outcomes. An effective measurement tool for the impact of health promotion on QoL has to be comprehensive and robust to capture the extent of physical, emotional, and social outcomes.(8)
Telemonitoring dramatically enhanced the health-related QoL (HRQoL) of 382 HF patients.(9) It used some scales and HRQoL using the EuroQol five dimensions questionnaire (EQ-5D) to determine functional status. The scores on the scale were not raised by telemonitoring. According to these results, telemonitoring helps HF patients' functional status and HRQoL. In Spain, the responsiveness of the questionnaire was evaluated using the Minnesota Living with HF Questionnaire (MLHFQ).(10) 1211 patients participated in the trial and answered the questionnaire both at baseline and six months after being released from the hospital. The findings demonstrated that the MLHFQ significantly affected QoL, with worsened patients experiencing losses, improved patients experiencing higher gains, and the same patients seeing lower gains. A meta-analysis found that mineralocorticoid receptor antagonists (MRAs) improved Left ventricular (LV) diastolic function in HF with conserved ejection fraction (HFpEF) patients, but did not lead to enhanced exercise capacity or QOL.(11)
The association between 90-day hospital readmissions in older patients with HF, activities of daily living (ADL), and nutritional condition was investigated.(12) According to the results, the readmission and non-readmission groups differed significantly in their body mass index (BMI), and hemoglobin. Additionally, some scores were found to be predictive of readmission within ninety days of discharge. Patients had a considerably decreased readmission avoidance rate. HF patients were more likely to experience cognitive impairment if patients have both physical frailty and depression, according to a South Korean research.(13) In cardiology outpatient clinics, 27,3 % of patients had cognitive impairment. The need for healthcare providers to understand the vulnerable demographic that had both physical frailty and depression was emphasized. The opinions of HF patients, medical professionals, and caregivers, about individual experiences, obstacles, and perceived needs, to the best possible care were investigated in a 2018 research carried out in Slovenia.(14) The results showed that limits, shifts in family responsibilities, and unpleasant emotional reactions were common subjects. Traditional food, lack of confidence, financial hardships, and lifestyle changes were all obstacles to self-care.
An educational intervention that affected depression and HF patients in rural areas was assessed.(15) The findings indicated that while self-care and knowledge about HF were enhanced in both intervention groups (int grp), health-related QoL was not. In individuals with depressed symptoms, no intervention effects were seen, and there were no variations in HRQOL between groups.
To evaluated health literacy, depression, self-care maintenance, Self-care, and confidence of HF Index (C-SCHFI).(16) The findings established a negative correlation among self-care management and depression, upholding, and confidence. The association among depression and self-care management was arbitrated by confidence and health literacy.
The goal of the research is to assess how well a six-stage self-management promotion model can improve HF patient's QoL. long-term effects were evaluated, and offer evidence for integrating multifaceted health promotion initiatives into clinical practice by addressing physical, emotional, and socioeconomic elements. The organization of the analysis: The next part explains the methodology section and then the result was provided. Next section gives the discussion and conclusion.
METHOD
This section outlines the methodology, including participant selection through stratified block sampling, the design of the Intervention group (int grp) and control group (ctrl grp), and the evaluation of QoL using specific variables. It also details the data analysis process, to assess differences in QoL scores between groups at different time points. The Flow of methodology is illustrated in figure 1.
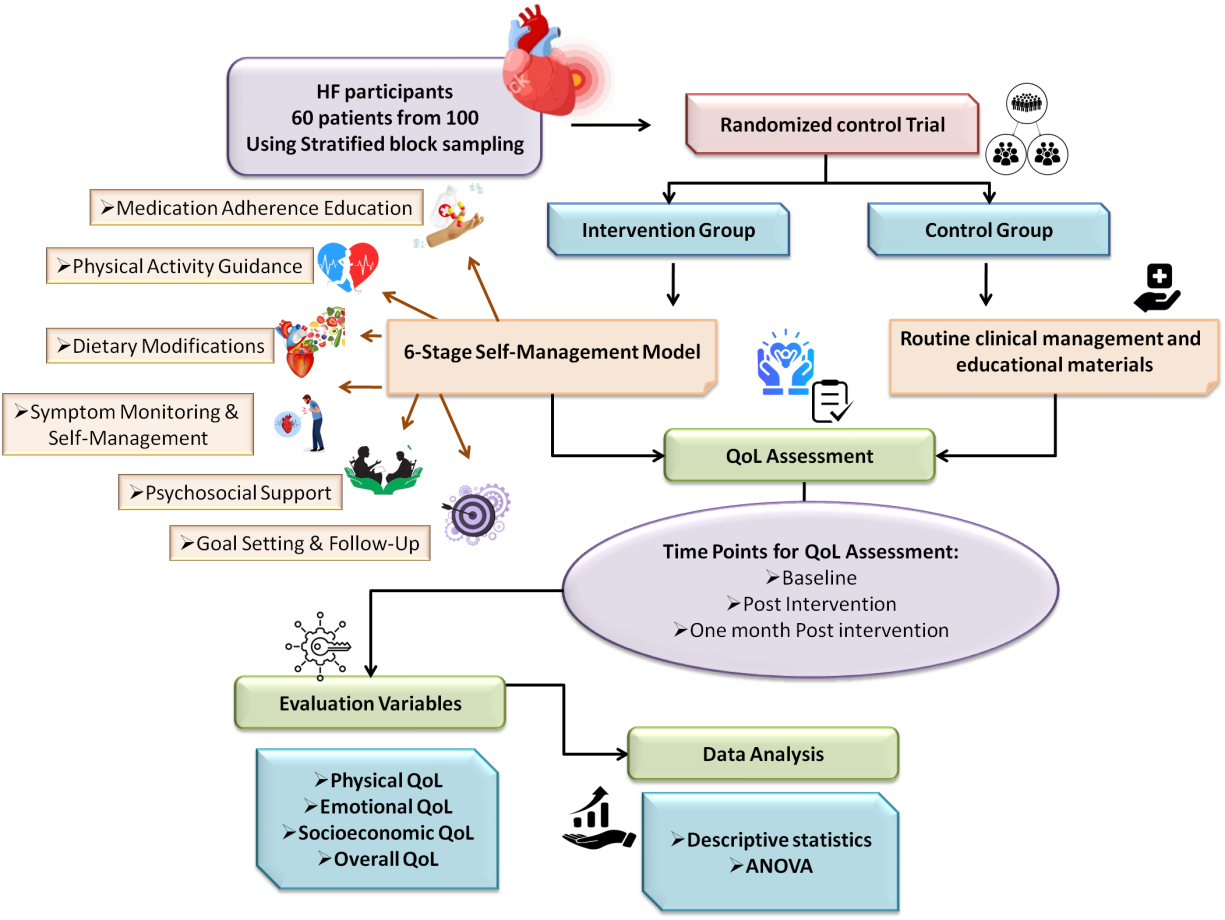
Figure 1. Method flow
Sample Selection
For this investigation, a total of 100 HF patients were initially considered. Using a stratified block sampling technique, a representative sample that captures the variability of the HF patient population was guaranteed. Using important factors like age, gender, and the severity of the disease, this approach separates the total patient population into discrete subgroups. 60 patients were selected for the final research from the 100-patient based on these filtered criteria, lowering potential biases and enabling a more accurate comparison between the groups. This sampling strategy improved the research sample's representativeness and made it possible to extrapolate the findings to a larger group of HF patients with different clinical and sociodemographic characteristics.
Participants Detail
Sixty HF patients divided equally into two groups: Int grp (30) and Ctrl grp(30). The patients were selected using structured survey. Table 1 provides the detailed demographic of the participants.
|
Table 1. Demographic details of HF patients |
|||
|
Demographic Characteristic |
Int Grp (n = 30) |
Ctrl Grp (n = 30) |
|
|
Age (mean ± SD) |
65,4 ± 8,2 years |
66,1 ± 7,5 years |
|
|
Sex |
Female |
14 (46,7 %) |
13 (43,3 %) |
|
Male |
16 (53,3 %) |
17 (56,7 %) |
|
|
Disease Severity |
Mild |
14 (46,7 %) |
13 (43,3 %) |
|
Moderate |
12 (40 %) |
14 (46,7 %) |
|
|
Severe |
4 (13,3 %) |
3 (10 %) |
|
|
Comorbidities |
Hypertension |
18 (60 %) |
19 (63,3 %) |
|
Diabetes |
12 (40 %) |
14 (46,7 %) |
|
|
Educational Level |
High school |
8 (26,7 %) |
9 (30 %) |
|
College/University |
22 (73,3 %) |
21 (70 %) |
|
|
Living Situation |
Alone |
7 (23,3 %) |
8 (26,7 %) |
|
With family |
23 (76,7 %) |
22 73,3 %) |
|
Randomized Controlled Trial (RCT)
The efficiency of the self-management promotion strategy in raising HF patients' QoL is assessed using an RCT design. Thirty patients each were randomly allocated to the int grp or ctrl groups out of 60 selected patients. Because each participant had an equal chance of being allocated to either group, the random allocation reduced selection bias and improved the reproducibility of results. Figure 2 illustrate the RCT.
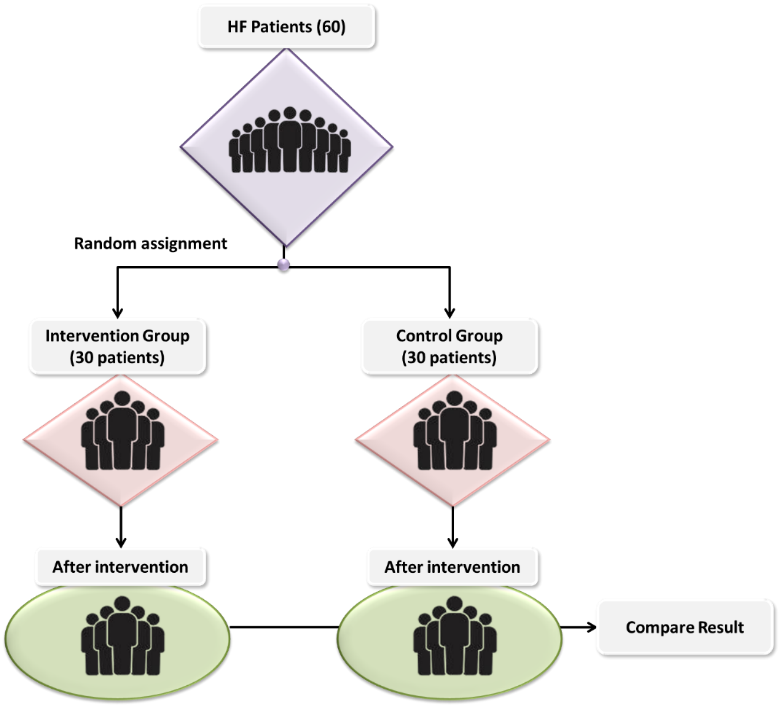
Figure 2. Randomized Control Trial illustration
Int Grp
A six-stage self-management promotion model was given to the int group to enhance their QoL. The goal of this all-inclusive paradigm was to emphasize both physical and mental health while addressing all facets of life with HF. The intervention's six phases were given below.
Medication Adherence Education: Participants received tailored counseling on medication types, possible adverse effects, appropriate dosages, and the significance of following prescribed regimens to enhance their comprehension and adherence to prescribed medications, which are essential in controlling HF. Additionally, resources like medication schedules and reminders were included.
Physical Activity Guidance: To encourage exercise while adhering to HF's restrictions to enhance cardiovascular health and general function. A customized workout regimen was created, beginning with easy exercises like walking and escalating in difficulty as needed. The program focused on strength training and cardiovascular exercises, which are good for HF patients.
Dietary Modifications: To promote heart health by diet, with an emphasis on a nutritious, low-sodium diet. Participants received education on healthy eating habits, such as how to increase fiber, decrease sodium intake, and have a balanced diet. Weekly meal plans and dishes catered to their dietary requirements were sent to them.
Symptom Monitoring and Self-Management: To enable people to keep an eye on their symptoms so patients can make better decisions about whether to get help. Instruction on observing symptoms daily (such as weight changes, edema, and dyspnea) and instructing patients on when and how to contact their healthcare professional for assistance.
Psychosocial Support: Addressing the psychological and emotional effects of HF can have a substantial impact on a patient's general health. Stress, anxiety, despair, and emotional distress were addressed through weekly group or individual counseling sessions. Additionally, coping mechanisms and relaxation techniques were provided.
Goal Setting and Follow-Up: To increase participation in the intervention and provide them with a sense of control over their health. Participants received guidance on how to develop objectives about their health-related habits. Follow-up conversations were conducted to assess progress, provide assistance, and discuss any issues.
Ctrl Grp
The Ctrl grp received standard care, which included routine medical management, periodic consultations, and access to general educational materials on HF management. These patients did not participate in the structured self-management program provided to the int grp. This allowed contrasting the effectiveness of the targeted self-management intervention with the standard care approach.
Research Instruments
QoL was assessed using a structured questionnaire consists of 24 questions with 5 point Likert scale (Never, rarely, sometimes, often, and always) tailored for HF patients at three critical time points.
Baseline: The initial assessment, conducted before the intervention began, served as the starting point to capture the patient's pre-intervention QoL levels.
Post-Intervention: The second assessment occurred immediately after the completion of the intervention program, enabling an evaluation of the immediate impact of the health promotion strategies on the patient's QoL.
Follow-Up: A third assessment was conducted one-month post-intervention to gauge the sustainability of the intervention's effects over time and examine whether improvements in QoL were maintained.
These time points allowed for an inclusive analysis of the short-term and potential long-term consequences of the health promotion intervention on HF patients' QoL. The structured questionnaire is provided in figure 3.
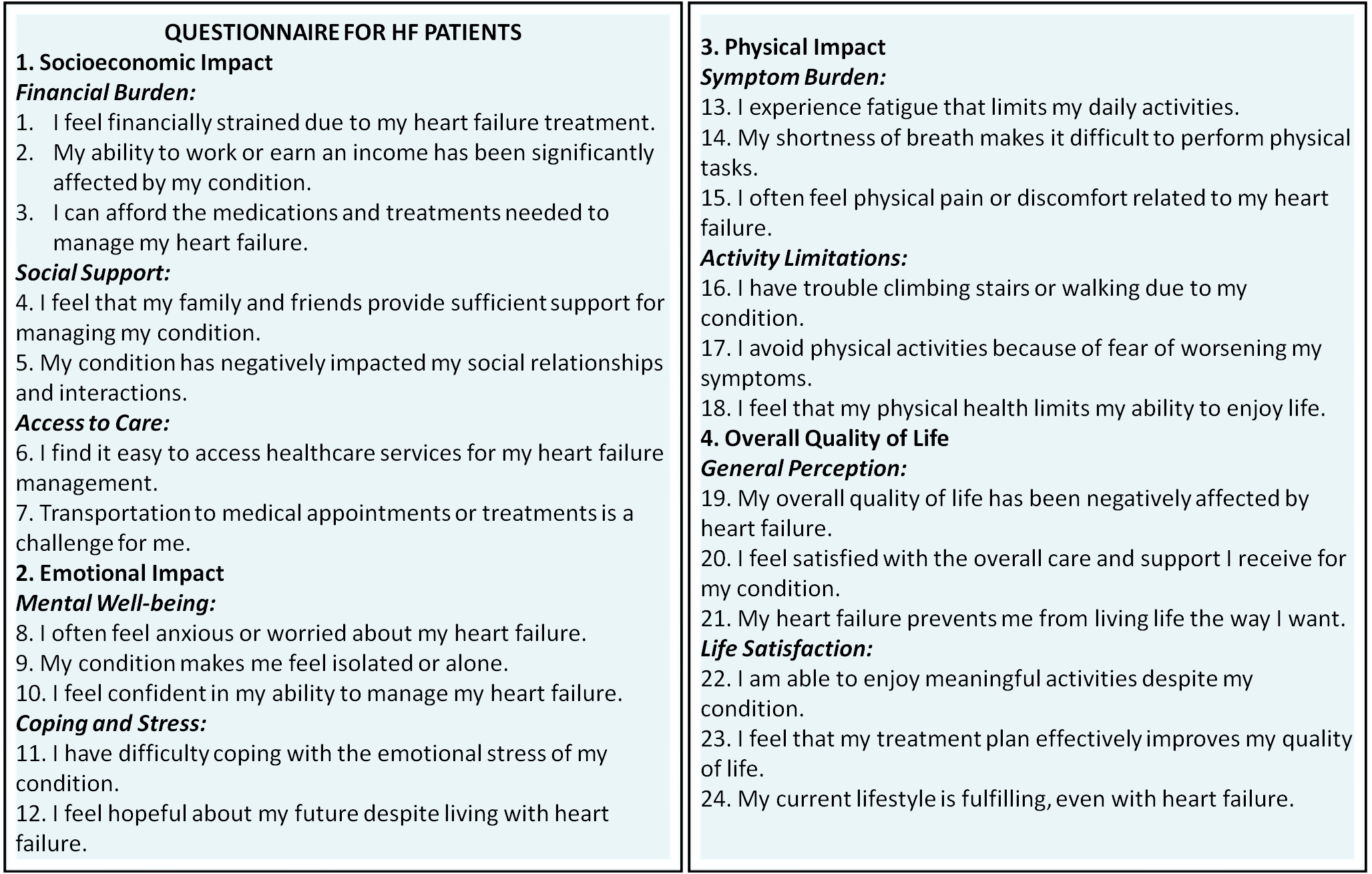
Figure 3. Questionnaire for assessing QoL of HF patients
Evaluation Variables
Four major variables were used in this research to evaluate QoL of socioeconomic, emotional, physical and overall QoL. Every category offered a thorough analysis of how the self-management promotion paradigm affected different facets of the patients' lives.
Physical: Evaluated the patient's physical health, including their general physical health, exercise tolerance, ability to carry out daily tasks, and medication adherence. Improvements in physical health brought about by the intervention would indicate a successful outcome because physical restrictions are frequently a major obstacle to maintaining a good QoL in HF patients.
Emotional: The emotional domain concentrates on the patient's psychological and emotional states, including stress, worry, and depression associated with their medical condition. It was anticipated that interventions targeted at enhancing emotional well-being (such as psychological support) would improve this element of QoL, as HF frequently results in emotional pain.
Socioeconomic: Evaluated things including job position, financial stability, and the capacity to control medical expenses. Financial stress can have a detrimental impact on QoL in individuals with long-term illnesses. Thus, the goal of the intervention was to increase patients' self-assurance in handling their illness, which may help their socioeconomic status by perhaps lowering hospital stays or health-related.
Overall QoL: Taking into account the psychological and physical effects of HF, this category offered a comprehensive evaluation of the patient's general health. The patient's perception of their health and overall QoL is reflected in the overall QoL score, which is a composite measure. It was assessed using the questionnaire, which also recorded the patients' perceived health condition and the impact of HF on day-to-day living.
Data Analysis
Using SPSS software, data analysis was carried out. To begin, descriptive statistics were computed to compile the participants' demographic and baseline characteristics. Analysis of variance (ANOVA) was to evaluate the variations in QoL scoresamong the int grp and ctrl grp at various intervals.
Descriptive statistics: It is a subfield of statistics that focus on resourcefully and methodically arranging, compressing, and displaying data. Without any conclusions or extrapolating to a broader population, it concentrates on characterizing and evaluating the key elements.
ANOVA: A statistical test used to assess the degree of difference among the average of more than two groups is used (Equation 1). ANOVA essentially makes it possible to contrast arithmetic means between groups simultaneously. ANOVA can determine if the observed differences reflect actual, meaningful changes or are the product of random chance.
![]()
(Note: MST and MSE stand for the Mean sum of squares due to treatment and error respectively; F-ANOVA coefficient)
RESULT
The descriptive statistics and ANOVA results for physical, emotional, socioeconomic, and overall QoL scores at three-time points are provided in this section. These analysis help to assess the impact of the intervention on various QoL domains across the int and ctrl grp. Figure 4 presents the questionnaire response percentages for physical, emotional, socioeconomic, and overall QoL at three-time points. The responses indicate improvements in all domains, suggesting that the self-management intervention had a positive result on the patient's QoL, with benefits maintained at follow-up.
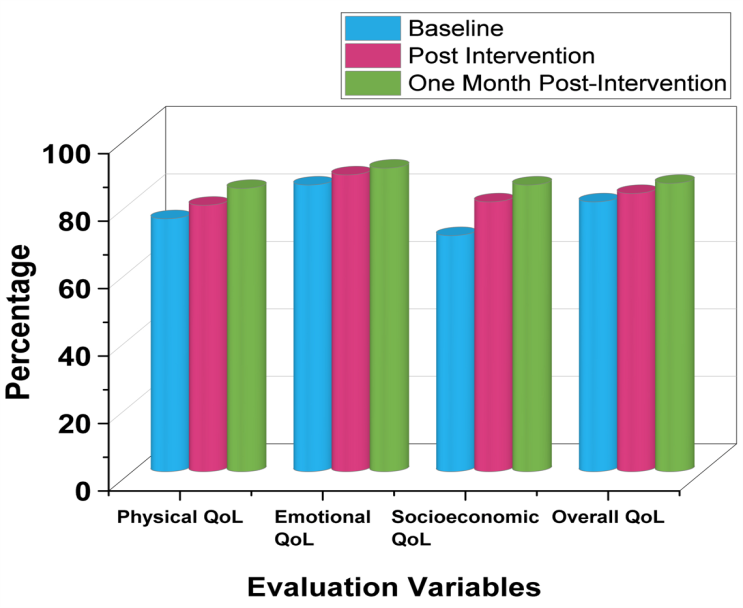
Figure 4. Questionnaire responses showing percentage improvement in QoL across four domains
Descriptive Statistics
Table 2 provides the descriptive statistics for the QoL subscales (Physical, Emotional, and Socioeconomic) and overall QoL at three-time points for both the int grp and ctrl grp. In the int grp, physical QoL decreased mean from 45,3 at baseline to 39,2 post-intervention and slightly further to 38,5 at one month post intervention, indicating a gradual decline in physical health. On the other hand, the ctrl grp showed relatively stable physical QoL mean (46,0 at baseline, 45,8 post-intervention, and 46,3 at one month post intervention). For emotional QoL, the int grp demonstrated a significant improvement, with scores dropping mean from 28,1 at baseline to 22,3 post-intervention and further to 20,4 at one month post intervention, suggesting that the intervention positively impacted emotional well-being. The ctrl grp’s emotional QoL remained relatively unchanged, moving from 27,5 at baseline to 27,3 at follow-up 22,3 postintervention. Regarding socioeconomic QoL (mean), the intervention group experienced a decline from 30,0 at baseline, 24,7 at post intervention and 23,6 at one month post intervention, while the ctrl grp’s scores fluctuated slightly but remained largely constant. Finally, overall QoL scores in the int grp reduced from 103,4 at baseline to 86,2 at post intervention and to 82,5 at one month post intervention, showing a general decline, which could be attributed to changes in the physical and socioeconomic subscales. The ctrl grp’s overall QoL remained nearly unchanged throughout the research period. Figure 5 gives the graphical representation of the mean score of Int grp and Ctrl grp.
|
Table 2. Descriptive Statistics for QoL Scores at three-time points |
||||
|
Evaluation Variable |
Group |
Baseline |
Post-Intervention |
One month post intervention |
|
Physical QoL |
Intervention |
45,3 ± 12,1 |
39,2 ± 10,4 |
38,5 ± 11,2 |
|
|
Control |
46,0 ± 13,2 |
45,8 ± 12,8 |
46,3 ± 13,1 |
|
Emotional QoL |
Intervention |
28,1 ± 9,7 |
22,3 ± 8,5 |
20,4 ± 7,9 |
|
|
Control |
27,5 ± 10,2 |
26,9 ± 9,6 |
27,3 ± 10,1 |
|
Socioeconomic QoL |
Intervention |
30,0 ± 8,4 |
24,7 ± 7,3 |
23,6 ± 6,9 |
|
|
Control |
31,2 ± 7,9 |
30,5 ± 8,2 |
31,0 ± 7,8 |
|
Overall QoL |
Intervention |
103,4 ± 28,4 |
86,2 ± 27,0 |
82,5 ± 25,1 |
|
|
Control |
104,7 ± 29,1 |
103,2 ± 28,5 |
104,6 ± 29,0 |
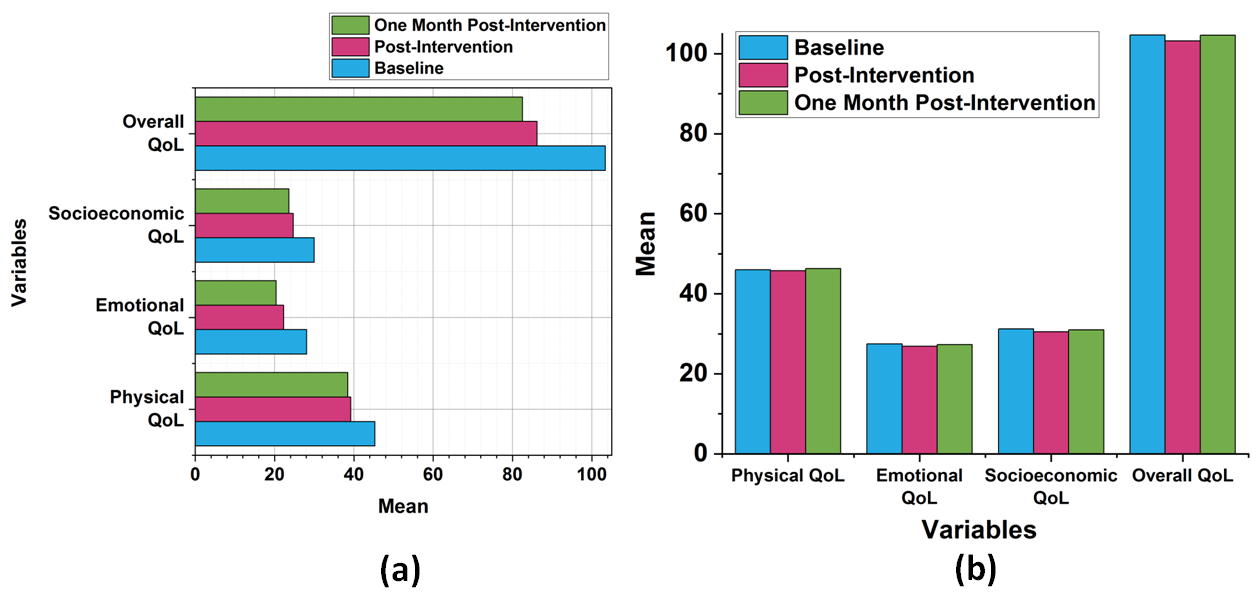
Figure 5. Mean score of (a) Int Grp and (b) Ctrl Grp
ANOVA Result
Table 3 displays the results of the ANOVA comparing QoL scores among the groups. The analysis reveals significant differences for physical QoL, with an F(8,56) and a p-measure of 0,0005, representing that the intervention had a measurable effect on physical QoL. Similarly, emotional QoL also proved a significant variation, with an F(4,72) and a p-measure of 0,014, signifying that the intervention had a positive effect on emotional well-being. However, the socioeconomic QoL subscale did not give a significant difference, with an F(3,01) and a p-measure of 0,057, representing that the intervention did not significantly improve this aspect of QoL. Finally, the overall QoL also gave a significant difference, with an F (9,24) and a p-measure of 0,0003, reflecting that the intervention had a significant impact on overall QoL, particularly driven by improvements in physical and emotional subscales.
|
Table 3. ANOVA Results for QoL Subscales |
|||||||
|
Evaluation Variable |
Source |
SS |
df |
MS |
F-Statistic (F) |
p-measure |
Interpretation |
|
Physical QoL |
Between groups |
350,2 |
2 |
175,1 |
8,56 |
0,0005 |
Significant |
|
Within groups |
1350 |
57 |
23,68 |
|
|
|
|
|
Total |
1700 |
59 |
|
|
|
|
|
|
Emotional QoL |
Between groups |
180,4 |
2 |
90,2 |
4,72 |
0,014 |
Significant |
|
Within groups |
1150 |
57 |
20,18 |
|
|
|
|
|
Total |
1330 |
59 |
|
|
|
|
|
|
Socioeconomic QoL |
Between groups |
140,5 |
2 |
70,25 |
3,01 |
0,057 |
Not Significant |
|
Within groups |
1140 |
57 |
20,00 |
|
|
|
|
|
Total |
1280 |
59 |
|
|
|
|
|
|
Overall QoL |
Between groups |
475,3 |
2 |
237,65 |
9,24 |
0,0003 |
Significant |
|
Within groups |
1800 |
57 |
31,58 |
|
|
|
|
|
Total |
2275 |
59 |
|
|
|
|
|
|
Note: MS – Mean square; SS- Sum of square; df – degrees of freedom |
|||||||
DISCUSSION
A structured self-management promotion paradigm may be useful in enhancing HF patients' QoL, especially in the emotional and physical domains. The value of including education on medication adherence, physical activity, and psychological support in health promotion efforts is shown by the int grp's notable gains in both physical and emotional QoL. These enhancements are consistent with the body of research that indicates focused interventions can enable patients to successfully manage their conditions. However, the lack of discernible progress in socioeconomic QoL would suggest that stronger support systems are required to deal with social and financial issues. While initial advantages are evident, the long-term sustainability of these gains merits more investigation, as evidenced by the lack of significant variation in overall QoL among the int grp and ctrl grp at particular periods. These findings highlight the necessity of incorporating multifaceted and long-term strategies to completely capture and improve heart failure patients' QoL.
CONCLUSIONS
The six-stage self-management promotion model can enhance the QoL of HF patients, particularly in the socio-economic sector was demonstrated. The structured questionnaire's overall QoL scores and different subscales did not significantly differ from the ctrl grp, although some subscales showed notable improvements inside the int grp. The complexity of HF patients' QoL and the challenges of achieving consistent gains in each domain are emphasized. Addressing the psychological and physical aspects of health is crucial, as demonstrated by the intervention's approach, which includes dietary modifications, medication adherence, physical activity, and psychosocial support and achieved the p value (<0,05). However, since there were no appreciable changes in overall QoL, longer follow-up periods and more targeted interventions may be needed to sustain and enhance the effects. Despite these limitations, provides valuable insights into how self-management practices can improve certain aspects of the QoL for HF patients. To enhance the long-term effectiveness of health promotion programs, future research should focus on larger, more diverse populations and explore new approaches. This will ensure comprehensive care that meets the various needs of individuals with HF.
BIBLIOGRAPHIC REFERENCES
1. Chicco D, Jurman G. Machine learning can predict survival of patients with heart failure from serum creatinine and ejection fraction alone. BMC medical informatics and decision making. 2020 Dec;20:1-6. https://doi.org/10.1186/s12911-020-1023-5
2. Johansson I, Joseph P, Balasubramanian K, McMurray JJ, Lund LH, Ezekowitz JA, Kamath D, Alhabib K, Bayes-Genis A, Budaj A, Dans AL. Health-related quality of life and mortality in heart failure: the global congestive heart failure research of 23 000 patients from 40 countries. Circulation. 2021 Jun 1;143(22):2129-42. 10.1161/CIRCULATIONAHA.120.050850
3. Erceg P, Despotovic N, Milosevic DP, Soldatovic I, Mihajlovic G, Vukcevic V, Mitrovic P, Markovic-Nikolic N, Micovic M, Mitrovic D, Davidovic M. Prognostic value of health-related quality of life in elderly patients hospitalized with heart failure. Clinical interventions in aging. 2019 May 22:935-45. https://doi.org/10.2147/CIA.S201403
4. Albuquerque de Almeida F, Al MJ, Koymans R, Riistama J, Pauws S, Severens JL. Impact of hospitalization on health-related quality of life in patients with chronic heart failure. Health and Quality of Life Outcomes. 2020 Dec;18:1-0. https://doi.org/10.1186/s12955-020-01508-8
5. Jönsson A, Cewers E, Ben Gal T, Weinstein JM, Strömberg A, Jaarsma T. Perspectives of health care providers on the role of culture in the self-care of patients with chronic heart failure: a qualitative interview research. International journal of environmental research and public health. 2020 Jul;17(14):5051. http://dx.doi.org/10.3390/ijerph17145051
6. Chew HS, Sim KL, Choi KC, Chair SY. Relationship between self-care adherence, time perspective, readiness to change and executive function in patients with heart failure. Journal of Behavioral Medicine. 2020 Aug;43:1-1. https://doi.org/10.1007/s10865-019-00080-x
7. Aamodt IT, Strömberg A, Hellesø R, Jaarsma T, Lie I. Tools to support self-care monitoring at home: perspectives of patients with heart failure. International journal of environmental research and public health. 2020 Dec;17(23):8916. http://dx.doi.org/10.3390/ijerph17238916
8. Massouh A, Skouri H, Cook P, Huijer HA, Khoury M, Meek P. Self-care confidence mediates self-care maintenance and management in patients with heart failure. Heart & Lung. 2020 Jan 1;49(1):30-5. https://doi.org/10.1016/j.hrtlng.2019.07.008
9. Gingele AJ, Ramaekers B, Brunner-La Rocca HP, De Weerd G, Kragten J, Van Empel V, Van Der Weg K, Vrijhoef HJ, Gorgels A, Cleuren G, Boyne JJ. Effects of tailored telemonitoring on functional status and health-related quality of life in patients with heart failure. Netherlands Heart Journal. 2019 Nov;27:565-74. https://doi.org/10.1007/s12471-019-01323-x
10. Gonzalez-Saenz de Tejada M, Bilbao A, Ansola L, Quirós R, García-Perez L, Navarro G, Escobar A. Responsiveness and minimal clinically important difference of the Minnesota living with heart failure questionnaire. Health and Quality of Life Outcomes. 2019 Dec;17:1-8. https://doi.org/10.1186/s12955-019-1104-2
11. Fukuta H, Goto T, Wakami K, Kamiya T, Ohte N. Effects of mineralocorticoid receptor antagonists on left ventricular diastolic function, exercise capacity, and quality of life in heart failure with preserved ejection fraction: a meta-analysis of randomized controlled trials. Heart and vessels. 2019 Apr 15;34:597-606. https://doi.org/10.1007/s00380-018-1279-1
12. Kitamura M, Izawa KP, Yaekura M, Mimura Y, Ikeda Y, Nagashima H, Brubaker PH. Relationship among activities of daily living, nutritional status, and 90 day readmission in elderly patients with heart failure. International journal of environmental research and public health. 2019 Dec;16(24):5068. http://dx.doi.org/10.3390/ijerph16245068
13. Lee JK, Won MH, Son YJ. Combined influence of depression and physical frailty on cognitive impairment in patients with heart failure. International journal of environmental research and public health. 2019 Jan;16(1):66. http://dx.doi.org/10.3390/ijerph16010066
14. Sedlar N, Lainscak M, Farkas J. Living with chronic heart failure: exploring patient, informal caregiver, and healthcare professional perceptions. International journal of environmental research and public health. 2020 Apr;17(8):2666. http://dx.doi.org/10.3390/ijerph17082666
15. Hwang B, Pelter MM, Moser DK, Dracup K. Effects of an educational intervention on heart failure knowledge, self-care behaviors, and health-related quality of life of patients with heart failure: Exploring the role of depression. Patient education and counseling. 2020 Jun 1;103(6):1201-8. https://doi.org/10.1016/j.pec.2020.01.007
16. Wang B, Xia L, Yu J, Feng Y, Hong J, Wang W. The multiple mediating effects of health literacy and self-care confidence between depression and self-care behaviors in patients with heart failure. Heart & Lung. 2020 Nov 1;49(6):842-7. https://doi.org/10.1016/j.hrtlng.2020.09.011
FINANCING
None.
CONFLICT OF INTEREST
None.
AUTHORSHIP CONTRIBUTION
Conceptualization: Renuka Jyothi. S, Suresh Kumar Behera, Indu Singh, Shankar Lal Soni.
Data curation: Renuka Jyothi. S, Suresh Kumar Behera, Indu Singh, Shankar Lal Soni.
Formal analysis: Renuka Jyothi. S, Suresh Kumar Behera, Indu Singh, Shankar Lal Soni.
Drafting - original draft: Renuka Jyothi. S, Suresh Kumar Behera, Indu Singh, Shankar Lal Soni.
Writing - proofreading and editing: Renuka Jyothi. S, Suresh Kumar Behera, Indu Singh, Shankar Lal Soni.